The failed vote in the U.S. Senate on the Dorgan Amendment to ‘allow’ lower-cost prescription medicines from licensed, registered pharmacies located in countries that have standards of oversight that meet or exceed those of the U.S. was both tragic and unnecessary.
It was tragic to watch the tremendous courage of Senator Byron Dorgan (D-ND), a man whom I greatly admire, who has been a champion of lowering prescription drug prices through ‘reimportation’ for nearly a decade, as he pleaded, cajoled and passionately made the point that the amendment was truly the only one that would have the effect of providing savings.
It was equally tragic to see him victimized by the deal-making of the Obama Administration with PhRMA. The snake that the President has decided to pick up may still bite him, as we warned in a previous entry.
At the same time, the spectacle was unnecessary. There are several reasons:
• As we have noted before, and even though we strongly support the right of personal importation, the bill, popularly called Dorgan-Snowe, was unworkable. It relied upon assumptions that simply were not possible to achieve:
• The first-year limitation upon medicines coming only from Canadian mail-order pharmacies was naive.
• There simply are not enough mail-order pharmacies left in Canada to provide the hoped-for funding;
• By restricting the ability to purchase medicines immediately from Australia, New Zealand and Great Britain for one year, and then limiting even those purchases to U.S.-based wholesalers and pharmacies, the bill’s supporters failed to acknowledge that as much as 80 percent of the sourcing for the Canadian mail-order pharmacies comes from Australia, New Zealand, and Great Britain.
• This was not the case when ‘reimportation’ first became an issue, but while the situation has changed, the language of the amendment reflected a situation that simply no longer exists, that of several years ago. It appears that the hoped-for impact was that since President Obama had co-sponsored a bill with virtually the same language two years ago, as had his Chief of Staff Rahm Emanuel on the House side, that they would be so flattered as to support the reincarnation of ‘their’ bill, a surprising bit of naivete.
• There was no opportunity for public input into the formation of the language. Supporters were given a ‘love it or Lump it’ choice. Some accepted this direction. I never did, not because I did not support the concept of importation, but because after years of hard work and support for personal importation, my responsibility remains the health benefits and savings that personal importation generates for seniors, workers, and others, not the mere passage of a bill.
• Many of the supporters of importation failed to ask themselves a very basic question: Why should Canada, which is a sovereign nation, and which through Health Canada has standards of oversight that meet or exceed those of the U.S. FDA, allow its pharmacies, operating completely within the laws of Canada and the provinces to be subject to U.S. inspections. Rather, why was there not a move made for reciprocal agreements?
But, in addition to being unworkable, there is another reason the amendment as written and the punishment heaped upon importation supporters was unnecessary: Importation of safe,affordable medicines is well-established through the common sense of the American public.
As the pharmaceutical industry continues to raise its prices, making deals with the Obama Administration that will lead to even greater costs for Medicare Part D payments by the government, growing numbers of Americans will be able to make wise, independent evaluations of safety and efficacy, as well as costs of medicines from safe, easily identifiable sources, not only from Canadian pharmacies, but through other pharmacies in Tier One Countries.
This is yet another example that all wisdom does not generate from within The Beltway but lies with the common sense of the American people.
For years, we have contended that individual, personal importation is allowed because the FDA itself has stated that a medicine that is not available in this country may be ordered in 90-day supplies for personal use, and any medicine that is not affordable is equally unavailable.
Also, that same common sense, enables Americans to evaluate the sources of their medicines for safety and efficacy as well as price. Those who believe that the FDA is the sole source of drug or product safety need to only look at the sorry record of the agency on a number of fronts ranging from Peanuts to Heparin.
As one who supported President Obama during his Presidential quest, I must admit to a deep sense of chagrin on a number of fronts. The deals with PhRMA are just the latest in a series of failed pledges for transparency and openness in government.
If Senator Dorgan wants to proceed with his quest, I encouraged him take actions that reflect the realities of the moment, rather than a bill with language that, while deserving support in a different time, is no longer relevant…irrespective, we shall increase our efforts to help the American people have the information to make informed, wise decisions, step forward, and exercise their common sense with the selection of safe, affordable medicines from pharmacies in other countries that meet or exceed the standards of those in the U.S.
Perhaps the President can then redeem himself by directing HHS to take steps to lead to reciprocal agreements with those countries for the benefit of the health care needs of untold numbers of people in this country. But, it is not necessary to wait for him or others within The Beltway to take action.
The American people have already spoken and as they are faced with the tremendous price increases initiated by pharma, we urge advocates of lower drug prices to help provide them with the information that will help them make the purchase decisions that will solidify the role of vital medicines in their healthcare regimen.

Making the case for personal importation of safe, affordable prescription medicines from licensed, registered pharmacies in Tier One Countries. Rx for American Health is published by Daniel Hines, an international award-winning communicator with five decades of experience, and the publisher of www.TodaysSeniorsNetwork.com and www.BoomersNewsOnline.com. He also works with progressive senior advocacy groups across the nation to promote the health and well-being of America’s aging population.
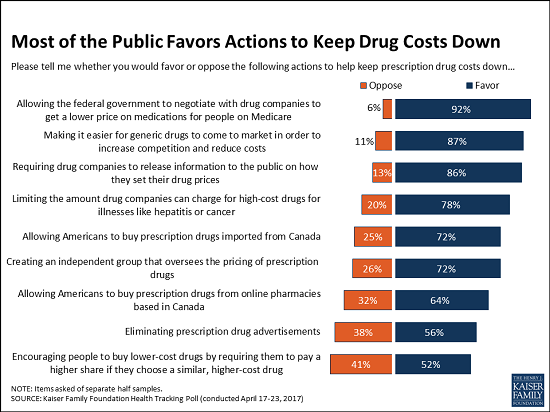
Kaiser Poll Show Support for Personal Imporatation
Wednesday, December 16, 2009
Monday, September 28, 2009
Has FDA reached its hubris with its disingenuous approach to justification of seizures of vital medicines, by thumbing its nose at Congress
Recent FDA seizures of individual purchases of vital, safe, affordable medicines from licensed, registered pharmacies in countries outside the U.S.—countries which have standards of oversight that meet or exceed those of the U.S. and our FDA—and statements made to justify such seizures illustrate that the agency has no appreciation or respect of the intent of Congress to end such seizures as well as engaging in disingenuous actions by claiming that any past Congressional actions do not apply to it. And, now, in an attempt to justify such seizures, it is evident that the Agency actually does not even know what actions Congress has taken in regard to personal importation of prescription medicines.
These are the inescapable conclusions after seizures recently started again. This prompted us to submit a series of inquiries to the FDA. The responses did not directly answer the questions. Now even more significantly, correspondence by the FDA to which we have gained access claims that "it is prohibited by congress (sic) to purchase prescription (sic) by mail."
Either the person making the statement is completely uninformed or is guilty of a deliberate falsehood.
As long ago as 2000, Congress approved the concept of 'reimportation', a misnomer since virtually no medicines are produced in the U.S. and the majority of prescriptions purchased in the U.S. is imported from other countries.
It was also passed in the last year of the Bush Administration, only to be turned away because it was attached to the FDA Reauthorization Bill, and President Bush had threatened a veto if the bill contained provisions for importation.
Added to this is the fact that for nearly a decade, personal importation has been supported by a huge number of sponsors in the House of Representatives and the Senate, only to be denied a vote because of parliamentary maneuvering by the highly effective pharmaceutical lobby.
That U.S. citizens should be denied access to vital, safe, affordable medicines via individual purchases for whatever reason best fits the moment for the FDA indicates that the agency, even in light of its failed record of safety for a number of products, is willing to allocate its limited resources to hindering personal importation.
One can only wonder whether such actions might actually do more harm to the people whose health it should be protecting by denying Americans access to personal importation as an integral part of their health regimen.
It is also reasonable to wonder whether or not seizing of safe, affordable medicines is done at the risk of detracting from seizures of counterfeit drugs from bogus pharmacies.
Some background is in order:
I have been and continue to be a strong supporter of personal importation. In that capacity I have worked—and continue to do so-- with seniors’ advocacy groups, policy-makers and as a communications consultant for companies that support importation of safe affordable medicines.
I have contacted and been in the offices of numerous Congressmen and Senators to make them aware of past actions by the FDA, Homeland Security and Customs in denying seniors and untold numbers of other Americans vital medicines that are important to the health and well-being of the persons ordering the medicines.
In 2006, we were successful in what, to that time, had been the to that time the most major abuse of power regarding seizures when elderly people across the country were not only having their medicines seized, but were receiving threatening letters from Customs officials telling the seniors that they were in violation of U.S. law.
This is, I and many others believe, a debatable point depending on one’s interpretation of the availability statement on the FDA’s own site saying that if a medicine or medical device is not available in this country, an individual may purchase it from outside the U.S.
My view is that if a medicine is unaffordable, it is certainly ‘unavailable’. Futher more, in an even more abusive attempt to scare America's elderly, in its letter, Customs went on to force the individuals to acknowledge that they knew they had violated U.S. law and were subject to prosecution if they continued to engage in such behavior, namely ordering medicines that helped keep them alive.
A sense of righteous indignation set in among elected officials. Then-Congressman Gil Gutknecht (R-MN) offered to file a friend of the court brief should supporters of importation decide that legal action be taken, his purpose being to illustrate how the FDA, Customs and Homeland Security were thumbing their nose at Congress. Senators Bill Nelson (D-FL) and David Vitter (R-LA) sponsored legislation to end the seizures, a clear signal that it did not approve of the actions of regulatory agencies designed to enforce the intent of the Legislative branch, not to design and interpret laws and make policy.
It was evident that the FDA was denying access to drugs that had not been tested for safety and efficacy. This is a crucial point since in the latest communications with FDA, the agency now (2009) says it does not have test results to affirm safety and efficacy. It does claim to have conduct tests and found ‘some drugs’ to not be authentic, but will not provide results from any tests it might have conducted on legitimate medicines. This leads to the inevitable conclusion that it has made its decisions whether to seize or not strictly upon country of origin rather than safety and efficacy
In 2006, the outrage over the seizures led to what was described as a ‘historic vote’ as the Senate took action, voting 68-32 to forbid such seizures. (And, herein lies the basis of the basis of the current disingenuous rationale of FDA…which now claims in verbatim statements that follow that the legislation was directed only towards Homeland Security, although the spokesperson for DHS at the time clearly states that the department was working in cooperation with FDA.
It is clear that the intent of the Congressional action—an intent which it clearly understood—was to defer seizures of specific medicines and pharmacies from acknowledged safe sources.
It was not aimed at hampering the seizures of counterfeit medicines from bogus pharmacies. Since the FDA, according to the comments of other agencies was cooperating in such seizures, this intent was directed equally towards all agencies involved in the seizures.
The issue seemed to be settled with the 2008 Presidential election. Both candidates supported importation of safe, affordable medicines from outside the U.S., and today, Senator John McCain (R-AZ) remains an outspoken advocate of importation.
Still, seizures have recently increased. This led us to make contacts with an FDA spokesperson to seek the rationale of the agency for the seizures. We had--and continue to have--several questions, including whether increased seizures might be a part of the deal struck by PhRMA to 'lower' the price and rate of increase of medicines in Medicare Part D's Doughnut Hole. That the claimed savings are illusionary and have been challenged by many policy-makers and advocates only adds to the suspicion that there might have been some 'quid pro quo' made by the Administration in return for PhRMA's 'cooperation.
But, it is an ill wind that blows now good. The responses to the series of inquiries and later statements made by other FDA officials in justifying seizures of personally imported medicines with a proven record of safety and efficacy, and absolutely no record of coming from bogus pharmacies or being counterfeit is illustrative of an agency that is suffering either from miscommunications in defense of its stance on such seizures, a complete lack of respect for the intent of the U.S. Congress, or a bias that indicates the unwillingness of the FDA to stick to its own guidelines as to its 'primary' reason for seizures--or all of the afore mentioned.
The FDA is a severely criticized agency. It has failed to protect American consumers from easily identifiable sources of potential contamination of on the medical front such as failure to identify defective medical devices from China. Even though it claims concern for drug safety, it failed to identify unsafe ingredients from China are blamed for deaths from Heparin, manufactured by Baxter.
It has also been criticized for failures in protecting the U.S. food supply for products ranging from domestically grown peanuts to imports of unsafe foods from China.
It is a matter of public record that the FDA has limited resources. So when we made our contact with a staffer assigned to deal with questions involving importation, our first question, submitted in writing was:
This is a typical Public Relations approach in which one answers a question that was not asked. It fails to address the question that was asked, and is nothing less than a tacit admission that the people making the seizures have no idea of the safety or efficacy of the medicines.
The agency has made a decision that it is doing more to promote drug safety by seizing individual purchases of medicines than to allocate its resources, which the FDA admits are limited, towards identifying bogus pharmacies and counterfeit drugs.
If the FDA needs help in identifying and distinguishing legitimate pharmacies from other countries, whose standards of quality meet or exceed those of the agency, surely a measured and more effective use of 'limited' resources could be expended in working for reciprocal arrangements to identify those pharmacies. If it needs help to identify bogus pharmacies, I suggest the agency cooperate with the Canadian International Pharmacy Association which has worked diligently to identify bogus pharmacies, or that it take advantage of several other sources that have done so.
Another question asked was about the 2006 vote:
This is, as noted above, completely disingenuous. In a statement at the time of the vote, the following statement was issued:
A Department of Homeland Security spokesperson in a statement said, "While we are reversing this policy, (Customs and Border Protection) remains committed, in cooperation with the FDA, to protecting the American public from unsafe and ineffective medications. We will be focusing our resources to best protect the American public." An FDA spokesperson declined to comment on the decision to end the seizures.
This statement makes the record clear. Congress had a clear intention to end seizures. At the time, the FDA declined comment, buy its silence spoke volumes in light of the admission by DHS that the policy was conducted in cooperation with the FDA.
While the spokesperson for FDA provided written answers, most of them were as follows:
This led to yet another question:
The response seems to indicate that the FDA has indeed tested and found problems with prescription medicines from the designated Tier One countries.
But the response to a specific request indicates that this is not the case.
The question follows:
The response follows:
And therein lies the self-imposed dilemma of the FDA.
It admits that it has not only has no reason for making seizures based on safety and efficacy of the legitimate vital medicines it has seized, but instead relies upon country of origin. Add to this, the attempts to twist the intent of Congress on forbidding such seizures, and the complete misstatement about Congress forbidding the purchase of prescriptions via mail. All lead to questions about the real intentions of the FDA.
And, we can only wonder if, while seizing vital medicines, how many shipments of counterfeit drugs from bogus pharmacies might have slipped past inspectors
These are the inescapable conclusions after seizures recently started again. This prompted us to submit a series of inquiries to the FDA. The responses did not directly answer the questions. Now even more significantly, correspondence by the FDA to which we have gained access claims that "it is prohibited by congress (sic) to purchase prescription (sic) by mail."
Either the person making the statement is completely uninformed or is guilty of a deliberate falsehood.
As long ago as 2000, Congress approved the concept of 'reimportation', a misnomer since virtually no medicines are produced in the U.S. and the majority of prescriptions purchased in the U.S. is imported from other countries.
It was also passed in the last year of the Bush Administration, only to be turned away because it was attached to the FDA Reauthorization Bill, and President Bush had threatened a veto if the bill contained provisions for importation.
Added to this is the fact that for nearly a decade, personal importation has been supported by a huge number of sponsors in the House of Representatives and the Senate, only to be denied a vote because of parliamentary maneuvering by the highly effective pharmaceutical lobby.
That U.S. citizens should be denied access to vital, safe, affordable medicines via individual purchases for whatever reason best fits the moment for the FDA indicates that the agency, even in light of its failed record of safety for a number of products, is willing to allocate its limited resources to hindering personal importation.
One can only wonder whether such actions might actually do more harm to the people whose health it should be protecting by denying Americans access to personal importation as an integral part of their health regimen.
It is also reasonable to wonder whether or not seizing of safe, affordable medicines is done at the risk of detracting from seizures of counterfeit drugs from bogus pharmacies.
Some background is in order:
I have been and continue to be a strong supporter of personal importation. In that capacity I have worked—and continue to do so-- with seniors’ advocacy groups, policy-makers and as a communications consultant for companies that support importation of safe affordable medicines.
I have contacted and been in the offices of numerous Congressmen and Senators to make them aware of past actions by the FDA, Homeland Security and Customs in denying seniors and untold numbers of other Americans vital medicines that are important to the health and well-being of the persons ordering the medicines.
In 2006, we were successful in what, to that time, had been the to that time the most major abuse of power regarding seizures when elderly people across the country were not only having their medicines seized, but were receiving threatening letters from Customs officials telling the seniors that they were in violation of U.S. law.
This is, I and many others believe, a debatable point depending on one’s interpretation of the availability statement on the FDA’s own site saying that if a medicine or medical device is not available in this country, an individual may purchase it from outside the U.S.
My view is that if a medicine is unaffordable, it is certainly ‘unavailable’. Futher more, in an even more abusive attempt to scare America's elderly, in its letter, Customs went on to force the individuals to acknowledge that they knew they had violated U.S. law and were subject to prosecution if they continued to engage in such behavior, namely ordering medicines that helped keep them alive.
A sense of righteous indignation set in among elected officials. Then-Congressman Gil Gutknecht (R-MN) offered to file a friend of the court brief should supporters of importation decide that legal action be taken, his purpose being to illustrate how the FDA, Customs and Homeland Security were thumbing their nose at Congress. Senators Bill Nelson (D-FL) and David Vitter (R-LA) sponsored legislation to end the seizures, a clear signal that it did not approve of the actions of regulatory agencies designed to enforce the intent of the Legislative branch, not to design and interpret laws and make policy.
It was evident that the FDA was denying access to drugs that had not been tested for safety and efficacy. This is a crucial point since in the latest communications with FDA, the agency now (2009) says it does not have test results to affirm safety and efficacy. It does claim to have conduct tests and found ‘some drugs’ to not be authentic, but will not provide results from any tests it might have conducted on legitimate medicines. This leads to the inevitable conclusion that it has made its decisions whether to seize or not strictly upon country of origin rather than safety and efficacy
In 2006, the outrage over the seizures led to what was described as a ‘historic vote’ as the Senate took action, voting 68-32 to forbid such seizures. (And, herein lies the basis of the basis of the current disingenuous rationale of FDA…which now claims in verbatim statements that follow that the legislation was directed only towards Homeland Security, although the spokesperson for DHS at the time clearly states that the department was working in cooperation with FDA.
It is clear that the intent of the Congressional action—an intent which it clearly understood—was to defer seizures of specific medicines and pharmacies from acknowledged safe sources.
It was not aimed at hampering the seizures of counterfeit medicines from bogus pharmacies. Since the FDA, according to the comments of other agencies was cooperating in such seizures, this intent was directed equally towards all agencies involved in the seizures.
The issue seemed to be settled with the 2008 Presidential election. Both candidates supported importation of safe, affordable medicines from outside the U.S., and today, Senator John McCain (R-AZ) remains an outspoken advocate of importation.
Still, seizures have recently increased. This led us to make contacts with an FDA spokesperson to seek the rationale of the agency for the seizures. We had--and continue to have--several questions, including whether increased seizures might be a part of the deal struck by PhRMA to 'lower' the price and rate of increase of medicines in Medicare Part D's Doughnut Hole. That the claimed savings are illusionary and have been challenged by many policy-makers and advocates only adds to the suspicion that there might have been some 'quid pro quo' made by the Administration in return for PhRMA's 'cooperation.
But, it is an ill wind that blows now good. The responses to the series of inquiries and later statements made by other FDA officials in justifying seizures of personally imported medicines with a proven record of safety and efficacy, and absolutely no record of coming from bogus pharmacies or being counterfeit is illustrative of an agency that is suffering either from miscommunications in defense of its stance on such seizures, a complete lack of respect for the intent of the U.S. Congress, or a bias that indicates the unwillingness of the FDA to stick to its own guidelines as to its 'primary' reason for seizures--or all of the afore mentioned.
The FDA is a severely criticized agency. It has failed to protect American consumers from easily identifiable sources of potential contamination of on the medical front such as failure to identify defective medical devices from China. Even though it claims concern for drug safety, it failed to identify unsafe ingredients from China are blamed for deaths from Heparin, manufactured by Baxter.
It has also been criticized for failures in protecting the U.S. food supply for products ranging from domestically grown peanuts to imports of unsafe foods from China.
It is a matter of public record that the FDA has limited resources. So when we made our contact with a staffer assigned to deal with questions involving importation, our first question, submitted in writing was:
Knowing of admittedly limited resources of the FDA, how does the agency reconcile the seizure of proven safe medicines from legitimate pharmacies (albeit from outside the U.S.) with the possibility that dispersing those limited resources might actually increase the chances of counterfeit medicines from bogus pharmacies escaping seizures.The answer such as it is follows:
"Because of limited resources the FDA uses a risk based approach to detention and actions related to imported drugs"
This is a typical Public Relations approach in which one answers a question that was not asked. It fails to address the question that was asked, and is nothing less than a tacit admission that the people making the seizures have no idea of the safety or efficacy of the medicines.
The agency has made a decision that it is doing more to promote drug safety by seizing individual purchases of medicines than to allocate its resources, which the FDA admits are limited, towards identifying bogus pharmacies and counterfeit drugs.
If the FDA needs help in identifying and distinguishing legitimate pharmacies from other countries, whose standards of quality meet or exceed those of the agency, surely a measured and more effective use of 'limited' resources could be expended in working for reciprocal arrangements to identify those pharmacies. If it needs help to identify bogus pharmacies, I suggest the agency cooperate with the Canadian International Pharmacy Association which has worked diligently to identify bogus pharmacies, or that it take advantage of several other sources that have done so.
Another question asked was about the 2006 vote:
Congress voted to end the seizure of prescription medicines from licensed, registered pharmacies via Canadian pharmacies. How does the FDA reconcile that intent of Congress with the broad brush approach that such imported medicines are subject to seizure? Does the FDA supersede the Congress in this instance?The response follows:
“What you are referring to was directed to DHS authority. Under the FDA's current authorities, most of these drugs are illegal and unapproved.”
This is, as noted above, completely disingenuous. In a statement at the time of the vote, the following statement was issued:
A Department of Homeland Security spokesperson in a statement said, "While we are reversing this policy, (Customs and Border Protection) remains committed, in cooperation with the FDA, to protecting the American public from unsafe and ineffective medications. We will be focusing our resources to best protect the American public." An FDA spokesperson declined to comment on the decision to end the seizures.
This statement makes the record clear. Congress had a clear intention to end seizures. At the time, the FDA declined comment, buy its silence spoke volumes in light of the admission by DHS that the policy was conducted in cooperation with the FDA.
While the spokesperson for FDA provided written answers, most of them were as follows:
“Under current law, these products are illegal. Sometimes FDA does test products, and we have found substandard and counterfeit drugs.”
This led to yet another question:
Is the reason for such seizures continue based upon the point of origin, or has the FDA conducted any tests on the seized medicines from such pharmacies as described in (2) to determine the efficacy, quality, safety of the affected medicines? If so, what are the results of such testing? (For the record, (2) refers to “vital prescription medicines from licensed, registered pharmacies in other countries who standards of oversight meet or exceed those of the FDA?”The response follows:
Under current law, these products are illegal. Sometimes FDA does test products, and we have found substandard and counterfeit drugs.
The response seems to indicate that the FDA has indeed tested and found problems with prescription medicines from the designated Tier One countries.
But the response to a specific request indicates that this is not the case.
The question follows:
This is a request for the specific findings of substandard and counterfeit drugs from any licensed registered pharmacy from outside the U.S.
The response follows:
FDA does not have that information to share. Testing typically performed by the FDA relates to the identity and content of the product, and not to the efficacy, quality and safety of those products.
And therein lies the self-imposed dilemma of the FDA.
It admits that it has not only has no reason for making seizures based on safety and efficacy of the legitimate vital medicines it has seized, but instead relies upon country of origin. Add to this, the attempts to twist the intent of Congress on forbidding such seizures, and the complete misstatement about Congress forbidding the purchase of prescriptions via mail. All lead to questions about the real intentions of the FDA.
And, we can only wonder if, while seizing vital medicines, how many shipments of counterfeit drugs from bogus pharmacies might have slipped past inspectors
Sunday, September 13, 2009
Questions arise about motives of Senator Vitter regarding stance on prohibiting seizures of imported medicines
The motives of Senator David Vitter (R-LA), one of the traditional supporters of importation of prescription medicines from outside the U.S., have come into question because of the Senator’s response to a question from a participant in a Town Hall meeting and the lack of response to inquiries made to the Senator’s office about reports of stepped-up activity of seizures of vital medicines from legitimate, registered pharmacies in Tier One countries—medicines intended for individual purchase by U.S. citizens.
Also, he has a record of supporting the rights of individual purchases of safe, affordable prescription medicines, and was a leader along with Senator Bill Nelson (D-FL) in passing legislation forbidding the seizure of prescription medicines in 2007. We worked closely with the staff on board at that time to support the legislation. He was known as being friendly to issues involving not only individual access to imported medicines but those affecting the elderly as well, serving on the Senate Select Committee on Aging. And, to add to his credentials, he was successful in pushing through Senate approval of legislation to prohibit funding being used to seize prescription medicines in the next budget year.
An admirable record, indeed. So what is the problem?
With his answer to a constituent’s question at a Town Hall meeting in which the questioner suggested that by supporting such legislation to prohibit seizures, the Senator was actually saying that because of lower-priced medicines being available from Canadian pharmacies (an issue we’ll discuss shortly because it does not reflect the realities of the current situation involving sourcing for legitimate Internet-based and mail order pharmacies), the Senator was actually commending the Canadian Healthcare System.
Senator Vitter’s replay was disingenuous, to say the least. Instead of reaffirming his support of the rights of individuals to make such purchases, he retreated to pandering to his audience, saying that his real goal was to force prices in
Oh yeah, and I have some beachfront property in
Perhaps the reason the Senator believes that even though he pushed his bill through the Senate that the real reason that it would not be in any final bill coming out of the Senate-House conference was that his colleagues know that his real motive is not to lower drug prices in this country by ensuring the right of access for individual purchases and increasing the options available, but is merely an unworkable attempt to walk on both sides of this issue.
This is disappointing because several years ago, we worked with previous staff in the Senator’s office, and enjoyed such an amiable relationship that we were invited to participate in a Senate Aging Committee hearing that the Senator was planning in
Still, because of the Senator's record as a supporter of personal importation of safe, affordable medicines, we extended an invitation to current staff to respond to questions about the seizure ban legislation and related issues. The staff has declined to respond, creating additional questions about the Senator’s commitment to importation, and even of his commitment to presenting his views to
Perhaps it is just as well. The Senator’s anti-seizure bill is unlikely to gain any traction and will not be a part of any Conference Committee agreement. This is unfortunate, especially in light of questions about what PhRMA received in return for its decision to cut prices for seniors in the Doughnut Hole. Did it ‘negotiate’ that there would be no price negotiation for Part D? Did it receive an understanding that there would be increased seizures of individual, personal orders of prescription medicines from outside the
A final note: Earlier, we mentioned that the Senator’s bill to halt funding for seizures of medicines is flawed. In that regard, it shares with the Dorgan-Snowe bill for importation of personal medicines a fatal fault because the language of both reflects reliance upon importation of prescription medicines from
The problems
(a) Where at one time there were more than 140 mail-order or internet pharmacies in
(b) The primary souring for the medicines dispensed by these is not
(c) Finally, the Senator’s response to the question from the Town Hall meeting raises serious questions about his commitment to the role of importation as a part of a strategy to lower prescription medicine prices in this country.
(d) His belief that his stance will destroy not only the Canadian Health Care pricing structure but that of the rest of the world by forcing other countries to raise their drug prices, and that pharma will respond by lowering prices in the U.S. because it is able to charge more in other countries would be laughable were it not yet another example of the inability of many of our elected officials to understand the role that personal importation of prescription medicines could play in reducing prices and healthcare reform.
Wednesday, September 9, 2009
Dear Mr. President...an appeal to President Obama for his healthcare speech
Dear Mr. President:
Once again, you have been placed at the crossroads of history. Tonight (September 9) you will have an opportunity to regain the impetus of the need for real change that was delivered to you by the American people last November.
As one who foresaw you as the next President long before others had even thought of it, I urge you to use this chance to reclaim the mantle of leadership which, unfortunately and disappointingly, you gave to the Congress and the shrillness of the Town Hall Meetings in August.
As you prepare your remarks and as you reassume the mantle of leadership that is unique to the Presidency, remember some important points:
o You are the only elected official who has subjected himself to the extreme scrutiny of the American people.
o You are the leader of the Democrat Party, and alone have a national vision that will address a multitude of problems, including but not limited to healthcare.
o The people who disrupted the democratic process of Town Halls are a shrill minority. Yes, there were those who have legitimate concerns, but there are two things that abhor a vacuum--nature and communications. Something will always fill the vacuum, and in the Summer of 2009, it was, unfortunately a small, albeit loud and disruptive, number of people with a particular agenda aimed directly at usurping the results of the past three elections.
So, Mr. President, here is my suggestion. Speak plainly, not professorial. Tell people what you are going to tell them, tell them and then tell them what you have told them.
Take the playing field of the 2010 elections away from those GOP House and Senate members who are already envisioning their elevated roles in a new Congress by making it clear that you are willing to layout your proposals, that the Democrat Party stands ready (at least in large part) to stand with you and on behalf of the American people who need and deserve affordable healthcare.
Then, stake your position. Let it be known that your confidence in the correctness of what you and others are doing is such that you have full faith in the ability of a majority of the American people to do the right thing.
This will provide a voice for those of us whom have believed in your ability to provide the leadership to implement needed change. It will also reflect your confidence in the basic goodness of the American people. And, it will show that you realize that your ability to govern is based upon continuing to merit the trust and support of the country.
With all best wishes,
Daniel Hines
Once again, you have been placed at the crossroads of history. Tonight (September 9) you will have an opportunity to regain the impetus of the need for real change that was delivered to you by the American people last November.
As one who foresaw you as the next President long before others had even thought of it, I urge you to use this chance to reclaim the mantle of leadership which, unfortunately and disappointingly, you gave to the Congress and the shrillness of the Town Hall Meetings in August.
As you prepare your remarks and as you reassume the mantle of leadership that is unique to the Presidency, remember some important points:
o You are the only elected official who has subjected himself to the extreme scrutiny of the American people.
o You are the leader of the Democrat Party, and alone have a national vision that will address a multitude of problems, including but not limited to healthcare.
o The people who disrupted the democratic process of Town Halls are a shrill minority. Yes, there were those who have legitimate concerns, but there are two things that abhor a vacuum--nature and communications. Something will always fill the vacuum, and in the Summer of 2009, it was, unfortunately a small, albeit loud and disruptive, number of people with a particular agenda aimed directly at usurping the results of the past three elections.
So, Mr. President, here is my suggestion. Speak plainly, not professorial. Tell people what you are going to tell them, tell them and then tell them what you have told them.
Take the playing field of the 2010 elections away from those GOP House and Senate members who are already envisioning their elevated roles in a new Congress by making it clear that you are willing to layout your proposals, that the Democrat Party stands ready (at least in large part) to stand with you and on behalf of the American people who need and deserve affordable healthcare.
Then, stake your position. Let it be known that your confidence in the correctness of what you and others are doing is such that you have full faith in the ability of a majority of the American people to do the right thing.
This will provide a voice for those of us whom have believed in your ability to provide the leadership to implement needed change. It will also reflect your confidence in the basic goodness of the American people. And, it will show that you realize that your ability to govern is based upon continuing to merit the trust and support of the country.
With all best wishes,
Daniel Hines
Saturday, August 8, 2009
President should have known pharma was a snake when he picked it up
For the past three weeks, we have posted blogs wondering what the payback of the Obama Administration was to PhRMA in return for its 'support' of 'price cutting' for Medicare Part D Doughnut Hole prices, generating a claimed $80 billion savings.
We were among the first to suggest that the pattern of backroom dealing violated Candidate Obama's pledges of greater transparency and openness in government, and an end to the special relationship between industry groups and policy-makers. We noted with regret that the President had invited healthcare industry groups, including PhRMA, the trade association for the pharmaceutical industry, headed by Billy Tauzin, the former-Louisiana Congressman who not only engineered the restriction against price negotiation in Part D before resigning his elected post shortly afterward to accept a $2 million annual salary position as head of PhRMA. To some, including me, it appears that a case might be made that there could be a conflict between representing a Congressional district while leading a legislative effort that was going to reap billions of dollars in benefits for an industry that was soon going to offer you a $2 million salary. This was why we bemoaned the new found alliance of the Obama Administration with PhRMA.
We asked: What is the payback to the industry? It is an honored guest at The White House; it is praised by the President as he speaks to Seniors, praising pharma's largess in reducing their pain with the 'offer' to reduce the cost of medicines for those stuck in The Doughnut Hole; it negotiates with Senator Max Baucus, (D-MT), chair of the influential Senate Finance Committee (and the recipient of large contributions from the healthcare industry); it has the audacity to 'demand' that the White House 'clarify' its 'agreement' that the Administration will 'honor' its agreed-to commitment to not allow price negotiation--and it gets its way, as the White House quickly falls in line, even to the point of having Press Secretary Robert Gibbs flounder as he had to admit he really didn't know the details.
But then, in a complete flip-flop, the next day, a new stance emerges, largely due to opposition from House members such as Rep. Henry Waxman, chair of the influential House Energy and Commerce Committee, which included price negotiation in its markup of HR3200. Waxman put it bluntly--neither he nor the Committee were bound by the negotiations with the Administration or with Senator Baucus.
Apparently others had the same concerns at about the same time we started asking questions about the relationship of this Administration with the pharmaceutical industry. There is an increasing number of stories asking questions about details of the agreement.
This is a fortunate turn of events. During the campaign, Candidate Obama made two pledges regarding prescription medicines: (a) to lower prices for Medicare by removing the restriction on price negotiation and (b) to allow Americans to expand their freedom of choice by legislation that would allow personal importation of safe, affordable medicines from licensed, registered pharmacies in Tier One countries, those that have standards of safety and efficacy that meet or exceed those of the United States.
It is interesting to note that earlier this year--at about the time that the White House was starting its outreach with industry reps, including PhRMA, that seizures by the FDA of vital medicines from Tier One countries picked up. The question must be asked, was this another part of the deal being cut with PhRMA? It is well-known that in addition, the other monster under the bed for PhRMA is importation of medicines at affordable prices. Interestingly, these are the same medicines that the industry ships into this country at prices 60 to 70 percent higher.
After a concerted effort,including appeals directly to the President by publishers of leading websites for seniors, and news releases about the seizures, they declined.
The continued concern about seizures was the reason that we hailed the successful legislative maneuvering of Senator David Vitter (R-LA) for an amendment restricting such seizures, a stance that reaffirmed the banning of such seizures by Congress in 2006. Still, even the Senator has said that he is not confident that the Amendment will stick in conference, perhaps reflecting the feeling that many share that the reach of pharma is such that it can have its way.
And therein lies the moral of the dilemma that the President faces. Will legislation affecting the price and availability of vital medicines be conducted in the bright sunlight of openness and opportunity for total and equal participation by all? Or will we be subjected to the special interests of groups such as PhRMA?
If it should be the latter, we would like to remind our elected policy-makers of the old tale that so amply illustrates the consequences of bad decisions...the fable of the snake and the little girl:
The moral of the fable is that things are not always as the seem. PhRMA has not shed its skin. Americans pay the highest prices for prescription medicine in the world. The industry's predatory pricing has contributed to the costs that now are the biggest obstacle to necessary healthcare reform, and the 'savings' of the brokered arrangement carry a heavy price...we can only hope that it will not be a snakebite that creates a climate of an industry group dictating to the Administration and Congress, thereby throwing into question the need for and benefits of healthcare reform.
We were among the first to suggest that the pattern of backroom dealing violated Candidate Obama's pledges of greater transparency and openness in government, and an end to the special relationship between industry groups and policy-makers. We noted with regret that the President had invited healthcare industry groups, including PhRMA, the trade association for the pharmaceutical industry, headed by Billy Tauzin, the former-Louisiana Congressman who not only engineered the restriction against price negotiation in Part D before resigning his elected post shortly afterward to accept a $2 million annual salary position as head of PhRMA. To some, including me, it appears that a case might be made that there could be a conflict between representing a Congressional district while leading a legislative effort that was going to reap billions of dollars in benefits for an industry that was soon going to offer you a $2 million salary. This was why we bemoaned the new found alliance of the Obama Administration with PhRMA.
We asked: What is the payback to the industry? It is an honored guest at The White House; it is praised by the President as he speaks to Seniors, praising pharma's largess in reducing their pain with the 'offer' to reduce the cost of medicines for those stuck in The Doughnut Hole; it negotiates with Senator Max Baucus, (D-MT), chair of the influential Senate Finance Committee (and the recipient of large contributions from the healthcare industry); it has the audacity to 'demand' that the White House 'clarify' its 'agreement' that the Administration will 'honor' its agreed-to commitment to not allow price negotiation--and it gets its way, as the White House quickly falls in line, even to the point of having Press Secretary Robert Gibbs flounder as he had to admit he really didn't know the details.
But then, in a complete flip-flop, the next day, a new stance emerges, largely due to opposition from House members such as Rep. Henry Waxman, chair of the influential House Energy and Commerce Committee, which included price negotiation in its markup of HR3200. Waxman put it bluntly--neither he nor the Committee were bound by the negotiations with the Administration or with Senator Baucus.
Apparently others had the same concerns at about the same time we started asking questions about the relationship of this Administration with the pharmaceutical industry. There is an increasing number of stories asking questions about details of the agreement.
This is a fortunate turn of events. During the campaign, Candidate Obama made two pledges regarding prescription medicines: (a) to lower prices for Medicare by removing the restriction on price negotiation and (b) to allow Americans to expand their freedom of choice by legislation that would allow personal importation of safe, affordable medicines from licensed, registered pharmacies in Tier One countries, those that have standards of safety and efficacy that meet or exceed those of the United States.
It is interesting to note that earlier this year--at about the time that the White House was starting its outreach with industry reps, including PhRMA, that seizures by the FDA of vital medicines from Tier One countries picked up. The question must be asked, was this another part of the deal being cut with PhRMA? It is well-known that in addition, the other monster under the bed for PhRMA is importation of medicines at affordable prices. Interestingly, these are the same medicines that the industry ships into this country at prices 60 to 70 percent higher.
After a concerted effort,including appeals directly to the President by publishers of leading websites for seniors, and news releases about the seizures, they declined.
The continued concern about seizures was the reason that we hailed the successful legislative maneuvering of Senator David Vitter (R-LA) for an amendment restricting such seizures, a stance that reaffirmed the banning of such seizures by Congress in 2006. Still, even the Senator has said that he is not confident that the Amendment will stick in conference, perhaps reflecting the feeling that many share that the reach of pharma is such that it can have its way.
And therein lies the moral of the dilemma that the President faces. Will legislation affecting the price and availability of vital medicines be conducted in the bright sunlight of openness and opportunity for total and equal participation by all? Or will we be subjected to the special interests of groups such as PhRMA?
If it should be the latter, we would like to remind our elected policy-makers of the old tale that so amply illustrates the consequences of bad decisions...the fable of the snake and the little girl:
A young girl was trudging along a mountain path, trying to reach her grandmother's house. It was bitter cold, and the wind cut like a knife. When she was within sight of her destination, she heard a rustle at her feet.
Looking down, she saw a snake. Before she could move, the snake spoke to her. He said, "I am about to die. It is too cold for me up here, and I am freezing. There is no food in these mountains, and I am starving. Please put me under your coat and take me with you."
"No," replied the girl. "I know your kind. You are a rattlesnake. If I pick you up, you will bite me, and your bite is poisonous.”
"No, no," said the snake. "If you help me, you will be my best friend. I will treat you differently."
The little girl sat down on a rock for a moment to rest and think things over. She looked at the beautiful markings on the snake and had to admit that it was the most beautiful snake she had ever seen.
Suddenly, she said, "I believe you. I will save you. All living things deserve to be treated with kindness."
The little girl reached over, put the snake gently under her coat and proceeded toward her grandmother's house.
Within a moment, she felt a sharp pain in her side. The snake had bitten her.
"How could you do this to me?" she cried. "You promised that you would not bite me, and I trusted you!"
"You knew what I was when you picked me up," hissed the snake as he slithered away.
The moral of the fable is that things are not always as the seem. PhRMA has not shed its skin. Americans pay the highest prices for prescription medicine in the world. The industry's predatory pricing has contributed to the costs that now are the biggest obstacle to necessary healthcare reform, and the 'savings' of the brokered arrangement carry a heavy price...we can only hope that it will not be a snakebite that creates a climate of an industry group dictating to the Administration and Congress, thereby throwing into question the need for and benefits of healthcare reform.
Wednesday, July 29, 2009
Where does the President Stand?
In the previous post, we note that the President during his comments to the AARP meeting, did not speak forcefully for price negotiation for prescription medicines in Part D, only indicating that further price reductions might be possible. On July 29 in Raleigh, he came out more forceful for price negotiation. Is a stronger statement on the right and value of personal importation of medicines next? And, what will be PhRMA's reaction to the following comment?
12:57 p.m. - A male doctor asks about the "high costs of prescription drugs in America." Obama says the U.S. spends 77 percent more for drugs than any other country. Says the prescription drug bill passed a few years back prohibited Medicare from negotiating with drug companies for lower prices, something that needs to be included in a new health care bill. Does laud the drug companies for offering lower costs as part on the ongoing negotiations in Congress.
Are we hostage to pharmaceutical industry
From the dictionary: hos·tage Pronunciation: \ˈhäs-tij\
Function: noun
Etymology: Middle English, from Anglo-French, from hoste
Date: 13th century
definition: a person held by one party in a conflict as a pledge pending the fulfillment of an agreement
In our previous blog, we questioned what the pharmaceutical industry might be getting from its 'cooperation' in reducing prices for seniors in the Part D Doughnut Hole. In his AARP 'Town Hall Meeting' July 28, President Obama seemed to indicate that while he believed that we could lower prices even more, he failed to explain how. Then he explained how without 'negotiating' with PhRMA, the industry's trade association, the drug manufacturers would 'fight' for every 'cent of profit' they are making...and could make.
What a regrettable state of affairs, an Administration and the U.S. Congress being held hostage by what arguably is the most powerful industry in the world. Unless reform is passed that further enriches the pharmaceutical industry, it will fight reform.
This leads us to ask what other tactics will pharma resort to if it doesn't get its way. And, what price will there be for its 'cooperation'? Already, price negotiation for prescription drugs, and personal importation of medicines from Tier One countries seem to have been kicked to the curb. But the fact remains: There is a proven record of safety and efficacy, as well as affordability of imported medicines providing vital medicines to Americans. Is restricting the ability of those untold numbers of Americans to purchase safe, affordable medicines from pharmacies in Tier One countries to be next, making it a clean sweep for pharma? The U.S. Congress has previously voted to end such questionable activity and most recently, Senator David Vitter (R-LA)has been successful with his introduction of legislation to prohibit such seizures for the next fiscal year. The chances of this being coming out of conference is uncertain. The Senator's office has declined to respond to inquiries about the amendment's prospects, but should it not be retained, the question must be asked, why. This is a legitimate question in light of pharma's success on a number of fronts, all the while claiming to exhibit a spirit of concern about what it does to lower prescription drug prices for Americans (the highest in the world), while holding a club of the threat of higher prices and withdrawal of its 'cooperation' in reaching an agreement.
Excerpts from the President's remarks follow:
Excerpt from opening remarks:
Function: noun
Etymology: Middle English, from Anglo-French, from hoste
Date: 13th century
definition: a person held by one party in a conflict as a pledge pending the fulfillment of an agreement
In our previous blog, we questioned what the pharmaceutical industry might be getting from its 'cooperation' in reducing prices for seniors in the Part D Doughnut Hole. In his AARP 'Town Hall Meeting' July 28, President Obama seemed to indicate that while he believed that we could lower prices even more, he failed to explain how. Then he explained how without 'negotiating' with PhRMA, the industry's trade association, the drug manufacturers would 'fight' for every 'cent of profit' they are making...and could make.
What a regrettable state of affairs, an Administration and the U.S. Congress being held hostage by what arguably is the most powerful industry in the world. Unless reform is passed that further enriches the pharmaceutical industry, it will fight reform.
This leads us to ask what other tactics will pharma resort to if it doesn't get its way. And, what price will there be for its 'cooperation'? Already, price negotiation for prescription drugs, and personal importation of medicines from Tier One countries seem to have been kicked to the curb. But the fact remains: There is a proven record of safety and efficacy, as well as affordability of imported medicines providing vital medicines to Americans. Is restricting the ability of those untold numbers of Americans to purchase safe, affordable medicines from pharmacies in Tier One countries to be next, making it a clean sweep for pharma? The U.S. Congress has previously voted to end such questionable activity and most recently, Senator David Vitter (R-LA)has been successful with his introduction of legislation to prohibit such seizures for the next fiscal year. The chances of this being coming out of conference is uncertain. The Senator's office has declined to respond to inquiries about the amendment's prospects, but should it not be retained, the question must be asked, why. This is a legitimate question in light of pharma's success on a number of fronts, all the while claiming to exhibit a spirit of concern about what it does to lower prescription drug prices for Americans (the highest in the world), while holding a club of the threat of higher prices and withdrawal of its 'cooperation' in reaching an agreement.
Excerpts from the President's remarks follow:
Excerpt from opening remarks:
"...And I think for AARP members especially there are hundreds of thousands of people out there who would directly benefit from reduced prescription drug costs if we're able to pass this bill.
And we'll work to close that doughnut hole in Medicare Part D that's costing so many folks so much money. Drug companies, as a consequence of our reform efforts, have already agreed to provide deeply discounted drugs, which will mean thousands of dollars in savings for the millions of seniors paying full price when they can least afford it..."
In response to a question:
Q Hi, this is my first year in the doughnut hole, and it's quite a frightening thing to go through. I have Parkison's so I will be going through it year after year, and it looks like I could last about two years, and then all of my savings will be gone to the doughnut hole. So what do you intend to replace the doughnut hole with?
THE PRESIDENT: Well, we want to replace it with prescription drugs that won't force you to use up all your retirement.
When the original Medicare Part D was put forward -- first of all, it wasn't paid for, so it automatically was unstable financially. Then there was an agreement that you couldn't negotiate with the drug companies for the cheapest available price on drugs. The American people pay about 77 percent more for drugs than any other country -- 77 percent. Almost twice as much as other countries do.
So what we've said is, as part of reform, let's negotiate with the pharmaceutical companies; we'll cover more people -- that means potentially the pharmaceuticals will have more coverage -- or more customers -- but as part of the deal, they've got to start providing much better discounts on their drugs. They've already committed that if the health care reforms pass, they would provide $80 billion worth of discounts. That would be enough to cover about half of the doughnut hole.
So, right off the bat, right now, without further negotiations, the drug companies have already committed that they would reduce -- they would cut in half the costs that folks have to go through when they're in the doughnut hole right now. That's money directly in their pocket that could be in their retirement savings.
I think we can get potentially an even better deal than that, because we're overpaying 77 percent.
But the problem is if we don't get health care reform, the pharmaceutical industry is going to fight for every dime of profits that they're currently making -- and filling that doughnut hole is going to be very expensive because when the Medicare Part D was originally passed nobody put in provisions to pay for -- and so putting even more money into it at a time when Medicare may go bankrupt -- not "go bankrupt," but go into the red 10 years from now, that's a big problem. That's part of the reason why reform is so important.
Friday, July 24, 2009
What is pharma's motive, payback for its cooperation?
The plan negotiated between the Senate Finance Committee and PhRMA, the trade association for the pharmaceutical industry is becoming increasingly troublesome as the debate over healthcare reform continues to drag on and on.
Many people worried about the new-found spirit of cooperation by the pharmaceutical industry when it was a guest/participant with others in the medical/insurance and healthcare industry at The White House.
This was after all the industry that had benefited from the last-minute engineered by then-LA Congressman Billy Tauzin that excluded negotiations for Medicare Part D prescription medicines, gave us the legacy of The Doughnut Hole, and helped pharmaceutical companies gain windfall profits.
And, it was former Congressman Tauzin who became a poster boy for pharma payback when he was rewarded with the $2 million a year job as head of PhRMA.
During the election, candidate Obama supported price negotiation for Part D medicine prices, and personal importation of safe, affordable prescription medicines from licensed, registered pharmacies in Tier One countries. While in the Senate, he was even a co-sponsor of personal importation legislation and early in his administration provided budget support for importation.
Now, these positions seem to have been replaced with "outreach" to the drug companies, which have shown their appreciation by pledging to cooperate with health care reform, and even to reduce prescription drug prices for seniors in The Doughnut Hole by as much as $80 billion.
So sure of its position is PhRMA that during the President's meetings in Europe, with the Pope and then his African visit, that Tauzin boasted that at a meeting at The White House an unnamed aide had told him that importation might not be necessary since the industry was being so cooperative and that the other savings from the reforms might be so great as to make lower drug prices unnecessary.
In other words, even though pharma has imposed upon the American public the highest drug prices in the world, that's "OK" and it will be allowed to continue its predatory pricing rather than having to reduce prices.
It is a bold move by Tauzin to make statements about Administration policy. Our attempts to identify the source of the statement about no need for importation have elicited no reaction from The White House press office, even though we were promised two weeks ago that the inquiry had been directed to the proper people and that we would receive an answer. So much for transparency and open government.
We should have had an inkling of the possibility that an Obama administration might crumble on importation when, during the election, Dora Hughes, a medical advisor for the Obama campaign, said that the candidate, if elected, might be willing to change his position of support of importation.
At that time, we sought clarification from campaign spokespersons and were assured that candidate Obama's support of importation was as strong as ever.
Back to the present: policy-makers and many advocates continue to point to The Doughnut Hole offer by PhRMA as 'good' for seniors. But, there is confusion about details of the arrangement. And, as some have noted, by lowering prices for those in The Doughnut Hole, they will only be in many instances the same lower prices for a temporary time as the regular, everyday prices paid by citizens in other countries. Why shouldn't such prices be negotiated for all medicines.
The question must also be asked: Since there is a proven record of personal importation of safe, affordable medicines from licensed, registered pharmacies in Tier One Countries (those whose oversight and regulations of pharmaceutical medicines and pharmacies meet or even exceed those of the U.S, why shouldn't such personal importation be a part of public healthcare policy? Or has PhRMA, as indicated by Tauzin's statement after his White House meeting, negotiated restrictions on such importation, perhaps even seizures of vital medicines, which was banned by the U.S. Congress in 2006 and which has arisen more recently as Senator David Vitter (R-LA) successfully sponsored an amendment to ensure that U.S. customs is forbidden to engage in such seizures? Added to this, since the 'full price' as set by PhRMA will be credited towards satisfying The Doughnut Hole, it means that seniors who have been unable to purchase medicines while in the Hole will hopefully be able to continue their medications and will get out of The Doughnut Hole where they can has catastrophic coverage.
At that point, the medicines return to full price with the U.S. government paying 95 percent of full costs, generating a government-supported windfall for pharma. Is this what PhRMA negotiated with the U.S. Senate? And is this a part of the price we must pay for such 'cooperation?' In the next few postings, we show why this might only be the tip of the iceberg.
Many people worried about the new-found spirit of cooperation by the pharmaceutical industry when it was a guest/participant with others in the medical/insurance and healthcare industry at The White House.
This was after all the industry that had benefited from the last-minute engineered by then-LA Congressman Billy Tauzin that excluded negotiations for Medicare Part D prescription medicines, gave us the legacy of The Doughnut Hole, and helped pharmaceutical companies gain windfall profits.
And, it was former Congressman Tauzin who became a poster boy for pharma payback when he was rewarded with the $2 million a year job as head of PhRMA.
During the election, candidate Obama supported price negotiation for Part D medicine prices, and personal importation of safe, affordable prescription medicines from licensed, registered pharmacies in Tier One countries. While in the Senate, he was even a co-sponsor of personal importation legislation and early in his administration provided budget support for importation.
Now, these positions seem to have been replaced with "outreach" to the drug companies, which have shown their appreciation by pledging to cooperate with health care reform, and even to reduce prescription drug prices for seniors in The Doughnut Hole by as much as $80 billion.
So sure of its position is PhRMA that during the President's meetings in Europe, with the Pope and then his African visit, that Tauzin boasted that at a meeting at The White House an unnamed aide had told him that importation might not be necessary since the industry was being so cooperative and that the other savings from the reforms might be so great as to make lower drug prices unnecessary.
In other words, even though pharma has imposed upon the American public the highest drug prices in the world, that's "OK" and it will be allowed to continue its predatory pricing rather than having to reduce prices.
It is a bold move by Tauzin to make statements about Administration policy. Our attempts to identify the source of the statement about no need for importation have elicited no reaction from The White House press office, even though we were promised two weeks ago that the inquiry had been directed to the proper people and that we would receive an answer. So much for transparency and open government.
We should have had an inkling of the possibility that an Obama administration might crumble on importation when, during the election, Dora Hughes, a medical advisor for the Obama campaign, said that the candidate, if elected, might be willing to change his position of support of importation.
At that time, we sought clarification from campaign spokespersons and were assured that candidate Obama's support of importation was as strong as ever.
Back to the present: policy-makers and many advocates continue to point to The Doughnut Hole offer by PhRMA as 'good' for seniors. But, there is confusion about details of the arrangement. And, as some have noted, by lowering prices for those in The Doughnut Hole, they will only be in many instances the same lower prices for a temporary time as the regular, everyday prices paid by citizens in other countries. Why shouldn't such prices be negotiated for all medicines.
The question must also be asked: Since there is a proven record of personal importation of safe, affordable medicines from licensed, registered pharmacies in Tier One Countries (those whose oversight and regulations of pharmaceutical medicines and pharmacies meet or even exceed those of the U.S, why shouldn't such personal importation be a part of public healthcare policy? Or has PhRMA, as indicated by Tauzin's statement after his White House meeting, negotiated restrictions on such importation, perhaps even seizures of vital medicines, which was banned by the U.S. Congress in 2006 and which has arisen more recently as Senator David Vitter (R-LA) successfully sponsored an amendment to ensure that U.S. customs is forbidden to engage in such seizures? Added to this, since the 'full price' as set by PhRMA will be credited towards satisfying The Doughnut Hole, it means that seniors who have been unable to purchase medicines while in the Hole will hopefully be able to continue their medications and will get out of The Doughnut Hole where they can has catastrophic coverage.
At that point, the medicines return to full price with the U.S. government paying 95 percent of full costs, generating a government-supported windfall for pharma. Is this what PhRMA negotiated with the U.S. Senate? And is this a part of the price we must pay for such 'cooperation?' In the next few postings, we show why this might only be the tip of the iceberg.
Wednesday, July 15, 2009
Time for critics of importation to look closer to home
Our most recent posting, actually a reposting, of an earlier criticism of Dr. Marv Shepherd, who, in his role as Director of the Center for Pharmacoeconomic Studies and Chairman of the Pharmacy Administration Division at the University of Texas-Austin College of Pharmacy, warned about the dangers of prescription medicines sold via internet mail-order pharmacies, suggesting that anyone making such an order, risked getting unsafe and/or counterfeit medicines, prompted a response from one reader who suggested that we lacked the courage of our convictions because while the Doctor 'signed' his papers, we published anonymously.
The writer failed to notice that sections of our blog site clearly identified us as the publisher of the site, so we expanded our identification. Interestingly, the critic had signed his/her response, 'Anonymous'.
But to move on. Let's see how concerned Dr. Shepherd and others who make misleading charges in an attempt to discourage individual importation of safe, affordable medications from licensed registered pharmacies are about the safety standards of the pharmaceutical industry itself.
This news release from the Missouri Attorney General indicates how two leading manufacturers risked the safety of Americans by their failure to report negative effects of two medicines they produced.
It is especially interesting to note that the attorneys general of 36 states were involved in the 'settlement' with Merck and Schering-Plough, but look where the drugs come from--Singapore, where the companies had a joint venture, named somewhat uncreatively MSP-Singapore.
So here is our standing invitation to Dr. Shepherd to show that he is truly concerned about prescription drug safety and holding pharma accountable for honest, open communications.
Using the University's PR budget, we urge him to do a study on bad medicines foisted upon the American public. Identify the companies, the medicines, and the potential health impact of the deception of pharma. Then, issue a news release about the need to make sure that pharma doesn't endanger the health and well-being of Americans.
The release follows. It is evident that the health threat to U.S. citizens from the misinformation of pharma is more of a threat than personal importation of safe, affordable prescriptions from licensed, registered pharmacies in Tier One countries.
Attorney General Koster announces Missouri to receive $100,000 in
settlement with Merck and Schering-Plough
--drug companies slow to disclose negative drug-study results--
Jefferson City, Mo. -- Attorney General Chris Koster today
announced a multi-state settlement with Merck & Co. Inc, Shering-Plough
Corporation, and a joint venture of the two companies, MSP Singapore
Company, LLC.
“When pharmaceutical companies slow reports of negative
drug-study results they are as good as lying to the public,” Koster
said. “It is unconscionable that a drug company would withhold
information that physicians and their patients need to make good
health-care decisions,” Koster said. “The agreement with Merck and
Schering-Plough sends a strong message that this Attorney General’s
office will be vigilant on public health issues and that we will not
allow businesses to put profits before patients.”
The settlement resolves an investigation into the companies'
lengthy delay in releasing negative results from the clinical trial
called ENHANCE (Ezetimibe and Simvastatin in Hypercholsterolemia
Enhances Atherosclerosis Regression). In this study, the
cholesterol-lowering drug Vytorin (a combination of the drug Zetia and
simvastatin) was no more effective reducing formation of plaque in
carotid arteries than the cheap, generically available
cholesterol-lowering drug simvastatin. Although ENHANCE ended May 2006,
a partial reporting of negative results did not occur until January 2008
and complete results were not published until the following April.
Prior to release of study results, Vytorin had been heavily promoted in
direct-to-consumer advertisements.
The settlement terms that now apply to Vytorin and Zetia are
requirements to:
● Obtain pre-approval from FDA for all direct-to-consumer
television advertisements;
● Comply with FDA suggestions to modify drug advertising;
● Register clinical trials and post their results;
● Prohibit ghost writing of articles;
● Reduce conflicts of interest for Data Safety Monitoring
Boards that ensure the safety of
participants in clinical trials; and,
● Comply with detailed rules prohibiting the deceptive use
of clinical trials.
In addition to these terms, the companies agreed to pay the
investigation costs of the 36 states participating in the settlement.
Missouri will receive $100,000 for its work on the investigation.
The writer failed to notice that sections of our blog site clearly identified us as the publisher of the site, so we expanded our identification. Interestingly, the critic had signed his/her response, 'Anonymous'.
But to move on. Let's see how concerned Dr. Shepherd and others who make misleading charges in an attempt to discourage individual importation of safe, affordable medications from licensed registered pharmacies are about the safety standards of the pharmaceutical industry itself.
This news release from the Missouri Attorney General indicates how two leading manufacturers risked the safety of Americans by their failure to report negative effects of two medicines they produced.
It is especially interesting to note that the attorneys general of 36 states were involved in the 'settlement' with Merck and Schering-Plough, but look where the drugs come from--Singapore, where the companies had a joint venture, named somewhat uncreatively MSP-Singapore.
So here is our standing invitation to Dr. Shepherd to show that he is truly concerned about prescription drug safety and holding pharma accountable for honest, open communications.
Using the University's PR budget, we urge him to do a study on bad medicines foisted upon the American public. Identify the companies, the medicines, and the potential health impact of the deception of pharma. Then, issue a news release about the need to make sure that pharma doesn't endanger the health and well-being of Americans.
The release follows. It is evident that the health threat to U.S. citizens from the misinformation of pharma is more of a threat than personal importation of safe, affordable prescriptions from licensed, registered pharmacies in Tier One countries.
Attorney General Koster announces Missouri to receive $100,000 in
settlement with Merck and Schering-Plough
--drug companies slow to disclose negative drug-study results--
Jefferson City, Mo. -- Attorney General Chris Koster today
announced a multi-state settlement with Merck & Co. Inc, Shering-Plough
Corporation, and a joint venture of the two companies, MSP Singapore
Company, LLC.
“When pharmaceutical companies slow reports of negative
drug-study results they are as good as lying to the public,” Koster
said. “It is unconscionable that a drug company would withhold
information that physicians and their patients need to make good
health-care decisions,” Koster said. “The agreement with Merck and
Schering-Plough sends a strong message that this Attorney General’s
office will be vigilant on public health issues and that we will not
allow businesses to put profits before patients.”
The settlement resolves an investigation into the companies'
lengthy delay in releasing negative results from the clinical trial
called ENHANCE (Ezetimibe and Simvastatin in Hypercholsterolemia
Enhances Atherosclerosis Regression). In this study, the
cholesterol-lowering drug Vytorin (a combination of the drug Zetia and
simvastatin) was no more effective reducing formation of plaque in
carotid arteries than the cheap, generically available
cholesterol-lowering drug simvastatin. Although ENHANCE ended May 2006,
a partial reporting of negative results did not occur until January 2008
and complete results were not published until the following April.
Prior to release of study results, Vytorin had been heavily promoted in
direct-to-consumer advertisements.
The settlement terms that now apply to Vytorin and Zetia are
requirements to:
● Obtain pre-approval from FDA for all direct-to-consumer
television advertisements;
● Comply with FDA suggestions to modify drug advertising;
● Register clinical trials and post their results;
● Prohibit ghost writing of articles;
● Reduce conflicts of interest for Data Safety Monitoring
Boards that ensure the safety of
participants in clinical trials; and,
● Comply with detailed rules prohibiting the deceptive use
of clinical trials.
In addition to these terms, the companies agreed to pay the
investigation costs of the 36 states participating in the settlement.
Missouri will receive $100,000 for its work on the investigation.
Friday, July 10, 2009
It's Deja Vu All Over Again
Earlier, we noted our concern over the apparent bail-out by The White House regarding PhRMA's Billy Tauzin, as he smugly announced that TWH suggested that personal importation of safe, affordable medicines from licensed registered pharmacies in Tier One Countries, those generally recognized as having standards of safety and efficacy that meet or exceed those of the U.S., might no longer 'be necessary' because of the 'savings' provided by comprehensive health care reform.
If we needed any proof that it was the signal for a launch by the pharmaceutical industry and its friends against moves to provide such vital medicines and provide some pricing pressure upon the predatory tactics of pharma, it has been provided by an 'old reliable', Dr. Marv Shepherd, who has devoted years of campaigning against importation of vital medicines.
We first came across Dr. Shepherd some years ago when we were still so naive as to believe that we could reach out to correct the misstatements made by some against importation. We were told by the Doctor at that time that the comments (about Terrorist links to Canadian pharmacies) he had made were merely raised at a meeting he was attending, and he further implied that he had a limited exposure to the issue.
When we found out the true extent of his involvement in the 'issue', we had an attack of righteous indignation, and published the following blog on another site. Now, just today, Dr. Shepherd has resurfaced to attempt to scare to death (likely by not taking vital medicines they cannot otherwise afford) of those Americans seeking the health benefits of safe, affordable prescription medicines. As a public service, we reprint the earlier article. As you read the list of speaking engagements and topics, remember, this was by a man who purported to me that he had little involvement with the subject of importation...the article follows. We make no claims about any funding that might or might not have been provided, although the latest release comes from the University:
The Past Leaves a Trail
Yesterday, we posted our news release link and blog on the activities of Dr. Marv Shepherd, who heads up something called the Pharmacoeconomic Studies Center at the University of Texas, laying out his record of misdirection with his article claiming that prescription drugs from Canada were 'counterfeit' and helped fund terrorist activities.
That he also took the time to rap the Vitter-Nelson amendment, approved 68-32 by the U.S. Senate, forbidding the seizure of prescriptions from licensed, registered pharmacies, indicated to us that he was really just carrying water for the pharmaceutical companies.
We had given him a chance to clarify his position. He claimed in a telephone call that he had heard something about the issue (terrorist links) at a California meeting earlier this summer. A little more research shows just how deep his lack of credibility goes and further validates that he has for years been mouthing the position of the large drug companies.
Here, from his web site, is a listing of papers, interviews and presentations he has made on pharmcoeconomic studies, whatever in the blazes that it. To me it looks more like a long history of opposition to access to safe, affordable prescriptions from outside the U.S., even if they are form licensed, registered pharmacies subject to the oversight of their own country's regulatory bodies. Perhaps Shepherd should be talking more about the recent finding that the FDA directory of prescription medicines is severely outdated.
Notice the phrases in the titles...'threats', 'dangers', 'vulnerbility', 'safety concerns', 'myths', 'effects on quality of care', just to name a few. Also, in his presentation on the impact of the millions of dollars spent on advertising directly to consumers, his conclusion was "Even though every year the javascript:void(0)industry spends millions of dollars on DTCA of prescription dmgs we cannot conclude that it influences drug prices." It is obvious that Shepherd's latest parroting of drug company claims was just another in a long series of papers, studies, etc. that lack any true academic standing. It's a shame that the people of Texas allow such a proud university to be used by large drug companies.
If you need more proof, here's the list of presentations by Dr. Shepherd...you are free to draw your own conclusions...why was he talking about the myths of reimportation to the Deparatment of Defense, for example...but one that is evident is that Shepherd was less that forthright with me when he tried to explain away his interest in counterfeiting as something that he had just heard about and felt compelled to write on, but was actually continuing a role of many years:
Presentations by Dr. Marv Shepherd
1."Prescription Drug Importation" presented at the 2004 Health Care Conference, Texas Association of Business and Texas Business Group on Health, Dallas, TX, September 8, 2004.
2. "Counterfeit Medicines: The American Experience" presented at the World Congress of Pharmacy and Pharmaceutical Sciences 2004, 64 th Congress of the Federation of International Pharmacists, New Orleans, LA September 9, 2004
3. "Threat of Drug Importation" presented at the West Texas Pharmacists Association, Lubbock, TX, September 18, 2004.
4. "Issues in Drug Importation" presented at the Illinois Pharmacists Association Annual Meeting, Arlington Heights, IL September 19, 2004.
5. "Threat of Drug Importation" presented at the Western New York Society of Health System Pharmacists meeting, Buffalo, NY, September 16, 2004.
6."Hazards of Drug Importation" presented at the University of Texas College of Pharmacy, Legends of Pharmacy Open and Learning on the Links Continuing Education Program, Austin, TX, September 24, 2004
7. "Threats of Drug Importation and Vulnerability of Our Drug Distribution System," presented at Florida A&M University Forum Series, College of Pharmacy and Pharmaceutical Sciences, Tallahassee, FL, October 5, 2004.
8. "Threat of Drug Importation," presented at the ARMSRx Ease of In-Sourcing Conference, Tortola, Bristish Virgin Islands, October 10, 2004.
9."Integrity of the Drug Supply System: Threats of Counterfeit Pharmaceuticals" presented at the Academy of Managed Care 2004 Educational conference, Baltimore, MD, Oct 15, 2004
10. "Drug Importation and the Vulnerability of Our Drug Supply Chain," presented at the American Society of Health-System Pharmacists 2004 Management Conference for Leaders in Pharmacy, Chicago, IL, October18, 2004.
11."The Importation of Drugs," presented at the Annual Meeting of the American College of Clinical Pharmacists, Dallas, TX, October 26, 2004.
12. "Wakeup Call: A Perfect Storm is Brewing" presented at the District VII and VII NABP-AACP Annual Meeting, Las Vegas, NV, October 28, 2004.
13. "Threat of Drug Importation and the Vulnerability of Our Drug Distribution System," presented at the Federal Pharmacy Conference, University of Texas, College of Pharmacy, Austin, TX, November 5, 2004
14."Statement on Prescription Drug Importation," presented and submitted to the Texas Legislative Conservative Coalition Research Institute Conference, Austin, TX, November 9, 2004.
15."Safety Concerns regarding Imported Medications," presented at the Understanding Importation Impact on Health Care Outcomes Conference, Madison, WI, November 11, 2004.
16. "New Drugs in the Pipeline and New Generic Releases," presented at the Department of Defense Pharmacoeconomics and Pharmacy Benefit Conference, San Antonio, TX, January 11, 2005
17. "Myths of Drug Importation" presented at the Department of Defense, Pharmacoeconomics and Pharmacy Benefit Conference, San Antonio, TX, January 12, 2005
18. "Effects of Drug Importation on Quality of Care," presented at the Coalition of Rheumatologists Advocacy Conference: Impact of Pharmacy Programs on Access to Rheumatologic Care, San Francisco, CA, January 22, 2005.
19."Myths of Drug Importation," presented at the Federation of American Hospitals Conference, Washington, D.C., February 28, 2005.
20."Drug Industry: Importation and Reimportation of Drugs," presented at the College of Psychiatric and Neurologic Pharmacists Annual Conference, San Diego, CA, March 12, 2005.
21. "Myths of Drug Importation," presented at the Michigan Health and Safety Coalition Patient Safety Conference, Dearborn, MI, April 8, 2005.
22."Global Pharmaceutical Marketplace/Importation," presented at the Food Marketing Institute 18 th Annual Supermarket Pharmacy Conference, New Orleans, LA, April 12, 2005.
23."Patients at Risk: Illegal Importation and Counterfeiting of Drugs," presented the Texas Organization of Rural and Community Hospitals Conference, Dallas, TX, April14, 2005.
24."Update on the Medicare Part D Prescription Drug Program," present at the College of Pharmacy University of Texas, Advisory Council, April 15, 2005.
25."Safety of America's Drug Supply Chain," presented at the Illinois Council of Health System Pharmacists and the Missouri Society of Health-System Pharmacists Spring Meeting, St. Charles, MO, April 16, 2005.
26."Internet Drug Traffic and Diversion of Prescription Drugs," presented at the Train the Trainer Drug Conference, Drug Enforcement Administration, El Paso, TX, April 20, 2005
27. "Myths of Drug Importation," presented at the Drug Enforcement Administration (DEA) Train the Trainer Conference, El Paso, TX, April 20, 2005.
28."The Truth and Consequences of Drug Importation," presented at the New Jersey Society of Health-System Pharmacists Annual Meeting, New Brunswick, NJ, April 21, 2005.
29."Myths of Drug Importation," presented at Argus Health Systems, Kansas City, MO, April 28, 2005.
30. "Policy Implications: Drug Quality, Safety Issues and Threats from Imported Medications," presented at the International Drug Importation Conference, Institute of Health Law Studies, California Western School of Law, San Diego, CA, June 3, 2005.
31."Myths of Drug Importation," presented at the Rochester NY Physicians Meeting, Rochester NY, June 13, 2005.
32."Myths of Drug Importation," presented at the Pfizer Pharmaceutical Speaker Program, Williamsville, NY, June 14, 2005.
33."Drug Importation: Global and Mexico," presented at the Healthcare Distribution Management Association 2005 Distribution Management Conference & Expo, Orlando, FL, June 16, 2005.
34."Threats of Drug Importation and the Vulnerability of Our Drug Distribution System," presented at the Arizona Pharmacy Alliance Annual Meeting, Phoenix, AZ, June 18, 2005.
35. "Drug Importation and the Vulnerability of Drug Distribution System," presented at the PharmaCare 3 rd Party Administrators Annual Conference, New Port RI, July 11, 2005.
36. "Counterfeit Drugs and the Vulnerability of Our Drug Distribution System," presented at the Texas Academy of Family Physicians Annual Meeting, San Antonio, TX, August 15, 2005.
37. "Thoughts on the Future of Pharmacy," presented at the Annul Pharmacy Conference of the Texas Community Health Centers, Austin, TX, August 25, 2005.
Research Presentations
38. Dastani H and Shepherd MD, "Predictors of Compliance and Persistence to Statin Therapy Among Texas Medicaid Patients," poster presentation at the annual meeting of the International Society of Pharmacoeconomics and Outcomes Research, Washington DC, May 16, 2005.
39. Nair R, Shepherd MD, Barner J, Lawson K, Wilson J and Warner D, Evaluation of Factors Related to Diagnosis of Hyperlipidemia: The Roll of Direct-to-Consumer Advertising Expenditures, Health Insurance Coverage and Gender, poster presentation at the annual meeting of the International Society of Pharmacoeconomics and Outcomes Research, Washington DC, May 16, 2005.
40. Shah S, Novak S and Shepherd MD, Evaluation and Comparison of Different Models of Metabolic Syndrome Using Confirmatory Factor Analysis, poster presentation at the annual meeting of the International Society of Pharmacoeconomics and Outcomes Research, Washington DC, May 17, 2005.
41. Panjabi, SS and Shepherd MD, Confirmatory Factor Analysis of the Beck Depression Inventory, poster presentation at the annual meeting of the International Society of Pharmacoeconomics and Outcomes Research, Washington DC, May 17, 2005.
42. Dastani H Shepherd MD, and Sasane R, Compliance and Persistence to Statin Therapy Among Texas Medicaid Patients, presented at the annual meeting of the Academy of Managed Care Pharmacy, Denver, CO, April 22, 2005.
Publications:
43. Shepherd, MD, "Counterfeit Drugs and the Pharmacist's Responsibilities" CESolutions, ( http://www.cesolution.com/) 1-12.
44. Shepherd, MD, "Drug Quality: Safety Issues and Threats of Drug Importation," California Western Law Review/International Law Journal , Special Edition, Summer 2005. 77-88.
45. "Alternatives in Savings in Purchasing of Medications," The Senior News Source , Vol 7, Issue 2, April 15, 2005. p.1
"Examination of the Relationship of Direct-to-Consumer Advertising Expenditures and Drug Price," Drug Information Journal , Vol 39, No.1, 2005, 13-24.
ED-OP Articles
46. Shepherd MD, "U.S. Should Solve Its Own Problems" Vancouver Sun , November 2, 2004, A13.
Shepherd, MD, "Canada is Not the Answer" Chicago Sun Times , October 23, 2004
47. "What if Canada Says 'No' to US on Drug Importation" USA TODAY , December 29, 2004, A13.
Interviews
48. Bioworld Today, "Canada Considers Stopping U.S. from Importing Drugs," January 18, 2005
49. KTBB-AM - Tyler TX - Talk Radio Interview, Roger Gray Show, January 11, 2005
50. KCRS-Midland/Odessa -Talk Radio, Robert Hallmark Show, January 11, 2005
DFW Metro Networks -Dallas TX, Amber Browne, January 20, 2005
Cooking Lite Magazine
51.San Antonio Express News , Editorial Advisory Board, January 11, 2005.
52.Austin American Statesman , Editorial Advisory Board, January 18, 2005
53.Houston Chronicle , Editorial Advisory Board, February 2, 2005
54. News Press Conference at the Texas Capital on Drug Importation, April 6, 2005
Would anyone like to make book on what he talked about at the Editorial Advisory Boards and the talk shows? I wish I had his frequent flyer miles since he has been all over the country...almost always protecting the position of large pharmaceutical companies. What in the world did he have to say to Pfizer, though?
If we needed any proof that it was the signal for a launch by the pharmaceutical industry and its friends against moves to provide such vital medicines and provide some pricing pressure upon the predatory tactics of pharma, it has been provided by an 'old reliable', Dr. Marv Shepherd, who has devoted years of campaigning against importation of vital medicines.
We first came across Dr. Shepherd some years ago when we were still so naive as to believe that we could reach out to correct the misstatements made by some against importation. We were told by the Doctor at that time that the comments (about Terrorist links to Canadian pharmacies) he had made were merely raised at a meeting he was attending, and he further implied that he had a limited exposure to the issue.
When we found out the true extent of his involvement in the 'issue', we had an attack of righteous indignation, and published the following blog on another site. Now, just today, Dr. Shepherd has resurfaced to attempt to scare to death (likely by not taking vital medicines they cannot otherwise afford) of those Americans seeking the health benefits of safe, affordable prescription medicines. As a public service, we reprint the earlier article. As you read the list of speaking engagements and topics, remember, this was by a man who purported to me that he had little involvement with the subject of importation...the article follows. We make no claims about any funding that might or might not have been provided, although the latest release comes from the University:
The Past Leaves a Trail
Yesterday, we posted our news release link and blog on the activities of Dr. Marv Shepherd, who heads up something called the Pharmacoeconomic Studies Center at the University of Texas, laying out his record of misdirection with his article claiming that prescription drugs from Canada were 'counterfeit' and helped fund terrorist activities.
That he also took the time to rap the Vitter-Nelson amendment, approved 68-32 by the U.S. Senate, forbidding the seizure of prescriptions from licensed, registered pharmacies, indicated to us that he was really just carrying water for the pharmaceutical companies.
We had given him a chance to clarify his position. He claimed in a telephone call that he had heard something about the issue (terrorist links) at a California meeting earlier this summer. A little more research shows just how deep his lack of credibility goes and further validates that he has for years been mouthing the position of the large drug companies.
Here, from his web site, is a listing of papers, interviews and presentations he has made on pharmcoeconomic studies, whatever in the blazes that it. To me it looks more like a long history of opposition to access to safe, affordable prescriptions from outside the U.S., even if they are form licensed, registered pharmacies subject to the oversight of their own country's regulatory bodies. Perhaps Shepherd should be talking more about the recent finding that the FDA directory of prescription medicines is severely outdated.
Notice the phrases in the titles...'threats', 'dangers', 'vulnerbility', 'safety concerns', 'myths', 'effects on quality of care', just to name a few. Also, in his presentation on the impact of the millions of dollars spent on advertising directly to consumers, his conclusion was "Even though every year the javascript:void(0)industry spends millions of dollars on DTCA of prescription dmgs we cannot conclude that it influences drug prices." It is obvious that Shepherd's latest parroting of drug company claims was just another in a long series of papers, studies, etc. that lack any true academic standing. It's a shame that the people of Texas allow such a proud university to be used by large drug companies.
If you need more proof, here's the list of presentations by Dr. Shepherd...you are free to draw your own conclusions...why was he talking about the myths of reimportation to the Deparatment of Defense, for example...but one that is evident is that Shepherd was less that forthright with me when he tried to explain away his interest in counterfeiting as something that he had just heard about and felt compelled to write on, but was actually continuing a role of many years:
Presentations by Dr. Marv Shepherd
1."Prescription Drug Importation" presented at the 2004 Health Care Conference, Texas Association of Business and Texas Business Group on Health, Dallas, TX, September 8, 2004.
2. "Counterfeit Medicines: The American Experience" presented at the World Congress of Pharmacy and Pharmaceutical Sciences 2004, 64 th Congress of the Federation of International Pharmacists, New Orleans, LA September 9, 2004
3. "Threat of Drug Importation" presented at the West Texas Pharmacists Association, Lubbock, TX, September 18, 2004.
4. "Issues in Drug Importation" presented at the Illinois Pharmacists Association Annual Meeting, Arlington Heights, IL September 19, 2004.
5. "Threat of Drug Importation" presented at the Western New York Society of Health System Pharmacists meeting, Buffalo, NY, September 16, 2004.
6."Hazards of Drug Importation" presented at the University of Texas College of Pharmacy, Legends of Pharmacy Open and Learning on the Links Continuing Education Program, Austin, TX, September 24, 2004
7. "Threats of Drug Importation and Vulnerability of Our Drug Distribution System," presented at Florida A&M University Forum Series, College of Pharmacy and Pharmaceutical Sciences, Tallahassee, FL, October 5, 2004.
8. "Threat of Drug Importation," presented at the ARMSRx Ease of In-Sourcing Conference, Tortola, Bristish Virgin Islands, October 10, 2004.
9."Integrity of the Drug Supply System: Threats of Counterfeit Pharmaceuticals" presented at the Academy of Managed Care 2004 Educational conference, Baltimore, MD, Oct 15, 2004
10. "Drug Importation and the Vulnerability of Our Drug Supply Chain," presented at the American Society of Health-System Pharmacists 2004 Management Conference for Leaders in Pharmacy, Chicago, IL, October18, 2004.
11."The Importation of Drugs," presented at the Annual Meeting of the American College of Clinical Pharmacists, Dallas, TX, October 26, 2004.
12. "Wakeup Call: A Perfect Storm is Brewing" presented at the District VII and VII NABP-AACP Annual Meeting, Las Vegas, NV, October 28, 2004.
13. "Threat of Drug Importation and the Vulnerability of Our Drug Distribution System," presented at the Federal Pharmacy Conference, University of Texas, College of Pharmacy, Austin, TX, November 5, 2004
14."Statement on Prescription Drug Importation," presented and submitted to the Texas Legislative Conservative Coalition Research Institute Conference, Austin, TX, November 9, 2004.
15."Safety Concerns regarding Imported Medications," presented at the Understanding Importation Impact on Health Care Outcomes Conference, Madison, WI, November 11, 2004.
16. "New Drugs in the Pipeline and New Generic Releases," presented at the Department of Defense Pharmacoeconomics and Pharmacy Benefit Conference, San Antonio, TX, January 11, 2005
17. "Myths of Drug Importation" presented at the Department of Defense, Pharmacoeconomics and Pharmacy Benefit Conference, San Antonio, TX, January 12, 2005
18. "Effects of Drug Importation on Quality of Care," presented at the Coalition of Rheumatologists Advocacy Conference: Impact of Pharmacy Programs on Access to Rheumatologic Care, San Francisco, CA, January 22, 2005.
19."Myths of Drug Importation," presented at the Federation of American Hospitals Conference, Washington, D.C., February 28, 2005.
20."Drug Industry: Importation and Reimportation of Drugs," presented at the College of Psychiatric and Neurologic Pharmacists Annual Conference, San Diego, CA, March 12, 2005.
21. "Myths of Drug Importation," presented at the Michigan Health and Safety Coalition Patient Safety Conference, Dearborn, MI, April 8, 2005.
22."Global Pharmaceutical Marketplace/Importation," presented at the Food Marketing Institute 18 th Annual Supermarket Pharmacy Conference, New Orleans, LA, April 12, 2005.
23."Patients at Risk: Illegal Importation and Counterfeiting of Drugs," presented the Texas Organization of Rural and Community Hospitals Conference, Dallas, TX, April14, 2005.
24."Update on the Medicare Part D Prescription Drug Program," present at the College of Pharmacy University of Texas, Advisory Council, April 15, 2005.
25."Safety of America's Drug Supply Chain," presented at the Illinois Council of Health System Pharmacists and the Missouri Society of Health-System Pharmacists Spring Meeting, St. Charles, MO, April 16, 2005.
26."Internet Drug Traffic and Diversion of Prescription Drugs," presented at the Train the Trainer Drug Conference, Drug Enforcement Administration, El Paso, TX, April 20, 2005
27. "Myths of Drug Importation," presented at the Drug Enforcement Administration (DEA) Train the Trainer Conference, El Paso, TX, April 20, 2005.
28."The Truth and Consequences of Drug Importation," presented at the New Jersey Society of Health-System Pharmacists Annual Meeting, New Brunswick, NJ, April 21, 2005.
29."Myths of Drug Importation," presented at Argus Health Systems, Kansas City, MO, April 28, 2005.
30. "Policy Implications: Drug Quality, Safety Issues and Threats from Imported Medications," presented at the International Drug Importation Conference, Institute of Health Law Studies, California Western School of Law, San Diego, CA, June 3, 2005.
31."Myths of Drug Importation," presented at the Rochester NY Physicians Meeting, Rochester NY, June 13, 2005.
32."Myths of Drug Importation," presented at the Pfizer Pharmaceutical Speaker Program, Williamsville, NY, June 14, 2005.
33."Drug Importation: Global and Mexico," presented at the Healthcare Distribution Management Association 2005 Distribution Management Conference & Expo, Orlando, FL, June 16, 2005.
34."Threats of Drug Importation and the Vulnerability of Our Drug Distribution System," presented at the Arizona Pharmacy Alliance Annual Meeting, Phoenix, AZ, June 18, 2005.
35. "Drug Importation and the Vulnerability of Drug Distribution System," presented at the PharmaCare 3 rd Party Administrators Annual Conference, New Port RI, July 11, 2005.
36. "Counterfeit Drugs and the Vulnerability of Our Drug Distribution System," presented at the Texas Academy of Family Physicians Annual Meeting, San Antonio, TX, August 15, 2005.
37. "Thoughts on the Future of Pharmacy," presented at the Annul Pharmacy Conference of the Texas Community Health Centers, Austin, TX, August 25, 2005.
Research Presentations
38. Dastani H and Shepherd MD, "Predictors of Compliance and Persistence to Statin Therapy Among Texas Medicaid Patients," poster presentation at the annual meeting of the International Society of Pharmacoeconomics and Outcomes Research, Washington DC, May 16, 2005.
39. Nair R, Shepherd MD, Barner J, Lawson K, Wilson J and Warner D, Evaluation of Factors Related to Diagnosis of Hyperlipidemia: The Roll of Direct-to-Consumer Advertising Expenditures, Health Insurance Coverage and Gender, poster presentation at the annual meeting of the International Society of Pharmacoeconomics and Outcomes Research, Washington DC, May 16, 2005.
40. Shah S, Novak S and Shepherd MD, Evaluation and Comparison of Different Models of Metabolic Syndrome Using Confirmatory Factor Analysis, poster presentation at the annual meeting of the International Society of Pharmacoeconomics and Outcomes Research, Washington DC, May 17, 2005.
41. Panjabi, SS and Shepherd MD, Confirmatory Factor Analysis of the Beck Depression Inventory, poster presentation at the annual meeting of the International Society of Pharmacoeconomics and Outcomes Research, Washington DC, May 17, 2005.
42. Dastani H Shepherd MD, and Sasane R, Compliance and Persistence to Statin Therapy Among Texas Medicaid Patients, presented at the annual meeting of the Academy of Managed Care Pharmacy, Denver, CO, April 22, 2005.
Publications:
43. Shepherd, MD, "Counterfeit Drugs and the Pharmacist's Responsibilities" CESolutions, ( http://www.cesolution.com/) 1-12.
44. Shepherd, MD, "Drug Quality: Safety Issues and Threats of Drug Importation," California Western Law Review/International Law Journal , Special Edition, Summer 2005. 77-88.
45. "Alternatives in Savings in Purchasing of Medications," The Senior News Source , Vol 7, Issue 2, April 15, 2005. p.1
"Examination of the Relationship of Direct-to-Consumer Advertising Expenditures and Drug Price," Drug Information Journal , Vol 39, No.1, 2005, 13-24.
ED-OP Articles
46. Shepherd MD, "U.S. Should Solve Its Own Problems" Vancouver Sun , November 2, 2004, A13.
Shepherd, MD, "Canada is Not the Answer" Chicago Sun Times , October 23, 2004
47. "What if Canada Says 'No' to US on Drug Importation" USA TODAY , December 29, 2004, A13.
Interviews
48. Bioworld Today, "Canada Considers Stopping U.S. from Importing Drugs," January 18, 2005
49. KTBB-AM - Tyler TX - Talk Radio Interview, Roger Gray Show, January 11, 2005
50. KCRS-Midland/Odessa -Talk Radio, Robert Hallmark Show, January 11, 2005
DFW Metro Networks -Dallas TX, Amber Browne, January 20, 2005
Cooking Lite Magazine
51.San Antonio Express News , Editorial Advisory Board, January 11, 2005.
52.Austin American Statesman , Editorial Advisory Board, January 18, 2005
53.Houston Chronicle , Editorial Advisory Board, February 2, 2005
54. News Press Conference at the Texas Capital on Drug Importation, April 6, 2005
Would anyone like to make book on what he talked about at the Editorial Advisory Boards and the talk shows? I wish I had his frequent flyer miles since he has been all over the country...almost always protecting the position of large pharmaceutical companies. What in the world did he have to say to Pfizer, though?
Thursday, July 9, 2009
Seniors Website Publisher expresses 'dismay' at purported White House stance on medicine reimportation
Publisher of leading information website for America's seniors,caregivers, advocates, policy-makers says purported White House stance on prescription medicine importation needs to be rebuked
Jul 08, 2009 – St. Louis, MO—The publisher of www.TodaysSeniorsNetwork.com, a leading informational website on aging issues for America’s seniors, caregivers, advocates and policy-makers, has expressed his ‘dismay’ at the announcement by a pharmaceutical industry representative that the Obama Administration has said that access to safe, affordable medications from licensed, registered pharmacies in Tier One countries might not be necessary to reduce the cost of prescription medicines for Americans.
Daniel Hines
, publisher of www.TodaysSeniorsNetwork.com, was responding to a statement by Billy Tauzin, president of the Pharmaceutical Research and Manufacturers of America (PhRMA) after an industry meeting with White House Staff, Tauzin is a former Louisiana Congressman, most noted as the Congressman who made possible provisions in Medicare Part D that ensured windfall profits and locked-in markets for the pharmaceutical industry, free of price negotiation, and establishing the ‘Doughnut Hole’. Upon resigning from Congress, Tauzin was named to his current PhRMA position at a $2 million annual salary.
“Tauzin implies that the White House believes that claimed savings of $80 billion over 10 years ‘negotiated’ with the Senate Finance Committee to reduce the costs of drugs sold to seniors in the Doughnut Hole, and other hoped for savings from comprehensive healthcare reform will be so great as to make individual importation ‘unnecessary’ “ Hines observes. “This is a fantasy that the American public should reject.”
Hines notes that the claimed Part D savings come on the heels of windfall profits made possible by price increases by the pharmaceutical industry over the life of Part D that have been so great as to force untold numbers of America’s elderly to either split their medications, or even quit taking vital medicines.
“:Also, the Congressional Budget Office is expected to score the drug companies’ ‘deal’ as saving far less than the claimed $80 billion,” Hines notes. “And, one must question, what is the leverage of the pharmaceutical industry to ‘negotiate’ legislation from the U.S. Congress, elected by the American citizenry.”
He urged President Obama to reaffirm his stance during the election campaign of support for the inclusion of individual purchases of safe, affordable prescription medicines from Tier One countries (those that are recognized as having standards of safety and oversight of licensed, registered pharmacies in their countries that meet or exceed those of the U.S. FDA).
“This could greatly reduce individual costs, while, at the same time, keeping the pharmaceutical industry ‘in-line’ rather than giving it a free-hand to raise prices and control supplies as it wishes,” Hines says. “By directing the Secretary of Health and Human Services to enter into some form of reciprocal arrangements, it would be possible to designate Tier One countries and to identify licensed pharmacies in those countries from which U.S. citizens may purchase their medicines, all the while confident of the safety and efficacy of the medicines, as well as the standards of the pharmacy filling the prescriptions.
“At the same time, the Administration should take two steps to further lower prescription prices: (1) Allow the inclusion of lower-cost personally imported prescription medicines into Part D plans to further lower costs to plan enrollees, generating savings for the government, and (2) keep its election campaign pledge to negotiate with the pharmaceutical industry, rather than accepting a deal by the industry to lower prices on the conditions of enactment of provisions within any legislation that will actually further increase and guarantee their markets at the expense of the American public.”
Jul 08, 2009 – St. Louis, MO—The publisher of www.TodaysSeniorsNetwork.com, a leading informational website on aging issues for America’s seniors, caregivers, advocates and policy-makers, has expressed his ‘dismay’ at the announcement by a pharmaceutical industry representative that the Obama Administration has said that access to safe, affordable medications from licensed, registered pharmacies in Tier One countries might not be necessary to reduce the cost of prescription medicines for Americans.
Daniel Hines
, publisher of www.TodaysSeniorsNetwork.com, was responding to a statement by Billy Tauzin, president of the Pharmaceutical Research and Manufacturers of America (PhRMA) after an industry meeting with White House Staff, Tauzin is a former Louisiana Congressman, most noted as the Congressman who made possible provisions in Medicare Part D that ensured windfall profits and locked-in markets for the pharmaceutical industry, free of price negotiation, and establishing the ‘Doughnut Hole’. Upon resigning from Congress, Tauzin was named to his current PhRMA position at a $2 million annual salary.
“Tauzin implies that the White House believes that claimed savings of $80 billion over 10 years ‘negotiated’ with the Senate Finance Committee to reduce the costs of drugs sold to seniors in the Doughnut Hole, and other hoped for savings from comprehensive healthcare reform will be so great as to make individual importation ‘unnecessary’ “ Hines observes. “This is a fantasy that the American public should reject.”
Hines notes that the claimed Part D savings come on the heels of windfall profits made possible by price increases by the pharmaceutical industry over the life of Part D that have been so great as to force untold numbers of America’s elderly to either split their medications, or even quit taking vital medicines.
“:Also, the Congressional Budget Office is expected to score the drug companies’ ‘deal’ as saving far less than the claimed $80 billion,” Hines notes. “And, one must question, what is the leverage of the pharmaceutical industry to ‘negotiate’ legislation from the U.S. Congress, elected by the American citizenry.”
He urged President Obama to reaffirm his stance during the election campaign of support for the inclusion of individual purchases of safe, affordable prescription medicines from Tier One countries (those that are recognized as having standards of safety and oversight of licensed, registered pharmacies in their countries that meet or exceed those of the U.S. FDA).
“This could greatly reduce individual costs, while, at the same time, keeping the pharmaceutical industry ‘in-line’ rather than giving it a free-hand to raise prices and control supplies as it wishes,” Hines says. “By directing the Secretary of Health and Human Services to enter into some form of reciprocal arrangements, it would be possible to designate Tier One countries and to identify licensed pharmacies in those countries from which U.S. citizens may purchase their medicines, all the while confident of the safety and efficacy of the medicines, as well as the standards of the pharmacy filling the prescriptions.
“At the same time, the Administration should take two steps to further lower prescription prices: (1) Allow the inclusion of lower-cost personally imported prescription medicines into Part D plans to further lower costs to plan enrollees, generating savings for the government, and (2) keep its election campaign pledge to negotiate with the pharmaceutical industry, rather than accepting a deal by the industry to lower prices on the conditions of enactment of provisions within any legislation that will actually further increase and guarantee their markets at the expense of the American public.”
Wednesday, June 24, 2009
Importation bill has chance to offer example of concern for ALL U.S. citizens, leadership, innovation
The news hit with the suddenness of a surprise attack early Saturday, June 20—the Pharmaceutical industry had made a late night call to Senator Max Baucus (D-MT) to tell him that is was willing to cooperate by pledging $80 billion over the next decade in resolving one of the biggest problems (and resulting criticisms) of Medicare Part D, The Infamous Doughnut Hole.
The facts surfaced by Monday afternoon however, as it became evident that pharma’s move really was nothing more than a carefully crafted and possibly successful attempt to circumvent several challenges facing it—the possibility of price negotiation for Part D medicines, and the potential contribution that could be provided by allowing personal importation of safe, affordable medicines from licensed, registered pharmacies in Tier One designated countries.
The Doughnut Hole should have been called ‘The Black Hole.’ Seniors were forced to continue paying their premiums, but their coverage was ‘suspended’ when drug costs reached $2250. They had entered The Doughnut Hole, where they would pay 100 percent of their prescriptions for the next $3600—even though they still had to pay for their premiums (a windfall for insurance companies). After paying the $3600, the ‘catastrophic’ level was reached, and the seniors who had survived The Doughnut Hole, were eligible for renewed coverage with low cost co-pays.
The fiscal and medical hit upon the elderly was immediate. Many seniors simply quit taking their medicines or began ‘splitting’ pills. Either action not only derailed the claimed hoped-for goals of Medicare Part D, it caused untold numbers of elderly to gamble their health, well-being and perhaps even their lives by the self-denial of vital medicines that had been forced on them by a pharmaceutical-influenced Congress that enacted Part D. Billy Tauzin, the former Congressman from New Orleans who was instrumental for many of the 11th hour (and 59 minute) changes that shaped Part D was rewarded with a multi-million-dollar position by PhRMA, the influential and well-heeled trade group for the drug companies.
A proposed solution to relieving the burden of The Doughnut Hole dilemma—price negotiation for drugs-- soon became a favorite of politicians, and repeated calls were made from untold numbers of stumps, town hall meetings, and locales where the pols could promise the elderly that help was on the way.
With the election of President Barack Obama, a Democratic House and a Democratic Senate, negotiation seemed ready to be moved from stump speeches to reality.
But, it is said that politics makes strange bedfellows. And, the push for healthcare reform soon created a lot of odd sleeping arrangements. Many of us winced when PhRMA joined with FamiliesUSA, a leading progressive, hard-working and well-respected advocacy group, to work for ‘healthcare reform.’ What, we asked, was the industry looking for? Images of the Fox in the Henhouse, the camel with his nose under the tent, flashed though our minds.
Added to this was the White House meeting President Obama arranged with industry groups representing insurance companies, PhRMA, hospitals, and other healthcare industry groups. Our concerns were quickly validated when a White House statement about pledges to cut the growth of health care costs was actually nothing more than a pledge to reduce the rate of growth by not increasing prices as much as before. The President needs to remember what John Kennedy said about big business special interest groups and what a bunch of SOBs they were.
The fact is that the ‘pledge’ was actually not a true savings. It would be a bit like buying your groceries at a store that has raised its prices 20 percent for the past few years. But, to ‘save money’, it says it will raise its prices only 10 percent next year, so instead of groceries that cost $100 per week in year one, the next year they would cost $110 instead of $120. The store owner could then tell consumers that each had saved $10 in year two, even though they were paying more for the same groceries. Only the rate of the increase was less than in previous years.
This type of math should have been the tip-off that the pharma ‘commitment’ to aiding seniors in The Doughnut Hole isn’t what it at first seemed to be.
On Sunday, President Obama issued the following statement about the agreement with the drug companies:
"I am pleased to announce that an agreement has been reached between Senator Max Baucus and the nation’s pharmaceutical companies that will bring down health care costs and reduce the price of prescription drugs for millions of America’s seniors. As part of the health reform legislation that I expect Congress to enact this year, pharmaceutical companies will extend discounts on prescription drugs to millions of seniors who currently are subjected to crushing out-of-pocket expenses when the yearly amounts they pay for medication fall within the doughnut hole any payments by seniors not covered by Medicare that fall between $2700 and $6153.75 per year. The existence of this gap in coverage has been a continuing injustice that has placed a great burden on many seniors. This deal will provide significant relief from that burden for millions of American seniors.
"The agreement by pharmaceutical companies to contribute to the health reform effort comes on the heels of the landmark pledge many health industry leaders made to me last month, when they offered to do their part to reduce health spending $2 trillion over the next decade. We are at a turning point in America’s journey toward health care reform. Key sectors of the health care industry acknowledge what American families and businesses already know - that the status quo is no longer sustainable. The agreement reached today to lower prescription drug costs for seniors will be an important part of the legislation I expect to sign into law in October. I want to commend House chairmen Henry Waxman, George Miller and Charles Rangel for addressing this issue in the health reform legislation they unveiled this week. This is a tangible example of the type of reform that will lower costs while assuring quality health care for every American."
It was to be Monday before the facts began to surface. Simply put, PhRMA had negotiated an arrangement that would become law only if Congress enacted comprehensive healthcare reform, a part of which would include expanded coverage for more Americans, creating new, additional and profitable markets for the pharmaceutical industry. It is distressing to once again witness the ability of pharma to define issues to its advantage. Perhaps I need a refresher course in civics, but why does the industry have to ‘agree’ to cuts that are intended to be a part of the governing legislation enacted by the U.S. Congress? What option do they have?
Also, why is the Obama Administration so ready to heap praises upon the drug companies, all of which have reaped whirlwind, virtually ensured profits at the expense of the American public that has been denied access to the health benefits provided by access to vital medicines because it must pay the highest cost in the world for its prescription medicines?
But, it is an ill-wind that blows no good. Last Fall, before the elections, a group of advocates for senior advocacy groups from areas across the country, met in Washington, DC to shape support for personal importation of prescription medicines from Tier One countries. At that time, the participants reached a consensus that the importation concept should be included as a part of discussion about comprehensive healthcare reform, a ‘third-leg’ of the stool, because such access to vital medicines is essential to the health and well-being of Americans. It also urged consideration of the beneficial budgetary impact that could be provided though the inclusion of personal importation of prescription medicines into Part D thereby remedying plan shortcomings while saving money for the elderly, protecting their health and creating real savings for the Plan.
Sources tell us that moves have made recently by supporters of importation to define a stronger argument for importation of prescription medicines within the framework of the healthcare debate. We applaud such action. Now, there is an additional opportunity to address the benefits of improved health and savings by fine-tuning the healthcare debate to explore other opportunities for personal importation and defining a role for personal importation in Medicare Part D. Senators Dorgan and Snowe, the two legislators most identified with importation, have issued a statement that reflects their realization that the pharma 'offer' really does not address the challenge of lowering prescription drug prices. And, already, there is a growing realization that the pharmaceutical industry's motives are self-serving.
It is time to call out the pharmaceutical industry. There are legitimate questions that deserve answers about the motives of pharma. It has reaped the benefits of guaranteed pricing for Part D that has led to windfall profits. The claimed or hoped-for savings,while beneficial to individuals, is too little-too late for many elderly. As to the claimed savings to be scored by the Congressional Budget Office, there is a growing realization that possible trade-offs to gain pharma support might actually lead to increased--and virtually guaranteed--sales and earnings.
There is a role for personal importation in helping provide a solution to providing safe, affordable prescription medicines for all Americans. We believe the pharma moves should lead to increased discussion of creating such access, free of what we believe to be unnecessary delays by empowering Secretary Sebelius to designate Tier One countries whose standards of oversight, safety, and efficacy meet of exceed those of the U.S.
The facts surfaced by Monday afternoon however, as it became evident that pharma’s move really was nothing more than a carefully crafted and possibly successful attempt to circumvent several challenges facing it—the possibility of price negotiation for Part D medicines, and the potential contribution that could be provided by allowing personal importation of safe, affordable medicines from licensed, registered pharmacies in Tier One designated countries.
The Doughnut Hole should have been called ‘The Black Hole.’ Seniors were forced to continue paying their premiums, but their coverage was ‘suspended’ when drug costs reached $2250. They had entered The Doughnut Hole, where they would pay 100 percent of their prescriptions for the next $3600—even though they still had to pay for their premiums (a windfall for insurance companies). After paying the $3600, the ‘catastrophic’ level was reached, and the seniors who had survived The Doughnut Hole, were eligible for renewed coverage with low cost co-pays.
The fiscal and medical hit upon the elderly was immediate. Many seniors simply quit taking their medicines or began ‘splitting’ pills. Either action not only derailed the claimed hoped-for goals of Medicare Part D, it caused untold numbers of elderly to gamble their health, well-being and perhaps even their lives by the self-denial of vital medicines that had been forced on them by a pharmaceutical-influenced Congress that enacted Part D. Billy Tauzin, the former Congressman from New Orleans who was instrumental for many of the 11th hour (and 59 minute) changes that shaped Part D was rewarded with a multi-million-dollar position by PhRMA, the influential and well-heeled trade group for the drug companies.
A proposed solution to relieving the burden of The Doughnut Hole dilemma—price negotiation for drugs-- soon became a favorite of politicians, and repeated calls were made from untold numbers of stumps, town hall meetings, and locales where the pols could promise the elderly that help was on the way.
With the election of President Barack Obama, a Democratic House and a Democratic Senate, negotiation seemed ready to be moved from stump speeches to reality.
But, it is said that politics makes strange bedfellows. And, the push for healthcare reform soon created a lot of odd sleeping arrangements. Many of us winced when PhRMA joined with FamiliesUSA, a leading progressive, hard-working and well-respected advocacy group, to work for ‘healthcare reform.’ What, we asked, was the industry looking for? Images of the Fox in the Henhouse, the camel with his nose under the tent, flashed though our minds.
Added to this was the White House meeting President Obama arranged with industry groups representing insurance companies, PhRMA, hospitals, and other healthcare industry groups. Our concerns were quickly validated when a White House statement about pledges to cut the growth of health care costs was actually nothing more than a pledge to reduce the rate of growth by not increasing prices as much as before. The President needs to remember what John Kennedy said about big business special interest groups and what a bunch of SOBs they were.
The fact is that the ‘pledge’ was actually not a true savings. It would be a bit like buying your groceries at a store that has raised its prices 20 percent for the past few years. But, to ‘save money’, it says it will raise its prices only 10 percent next year, so instead of groceries that cost $100 per week in year one, the next year they would cost $110 instead of $120. The store owner could then tell consumers that each had saved $10 in year two, even though they were paying more for the same groceries. Only the rate of the increase was less than in previous years.
This type of math should have been the tip-off that the pharma ‘commitment’ to aiding seniors in The Doughnut Hole isn’t what it at first seemed to be.
On Sunday, President Obama issued the following statement about the agreement with the drug companies:
"I am pleased to announce that an agreement has been reached between Senator Max Baucus and the nation’s pharmaceutical companies that will bring down health care costs and reduce the price of prescription drugs for millions of America’s seniors. As part of the health reform legislation that I expect Congress to enact this year, pharmaceutical companies will extend discounts on prescription drugs to millions of seniors who currently are subjected to crushing out-of-pocket expenses when the yearly amounts they pay for medication fall within the doughnut hole any payments by seniors not covered by Medicare that fall between $2700 and $6153.75 per year. The existence of this gap in coverage has been a continuing injustice that has placed a great burden on many seniors. This deal will provide significant relief from that burden for millions of American seniors.
"The agreement by pharmaceutical companies to contribute to the health reform effort comes on the heels of the landmark pledge many health industry leaders made to me last month, when they offered to do their part to reduce health spending $2 trillion over the next decade. We are at a turning point in America’s journey toward health care reform. Key sectors of the health care industry acknowledge what American families and businesses already know - that the status quo is no longer sustainable. The agreement reached today to lower prescription drug costs for seniors will be an important part of the legislation I expect to sign into law in October. I want to commend House chairmen Henry Waxman, George Miller and Charles Rangel for addressing this issue in the health reform legislation they unveiled this week. This is a tangible example of the type of reform that will lower costs while assuring quality health care for every American."
It was to be Monday before the facts began to surface. Simply put, PhRMA had negotiated an arrangement that would become law only if Congress enacted comprehensive healthcare reform, a part of which would include expanded coverage for more Americans, creating new, additional and profitable markets for the pharmaceutical industry. It is distressing to once again witness the ability of pharma to define issues to its advantage. Perhaps I need a refresher course in civics, but why does the industry have to ‘agree’ to cuts that are intended to be a part of the governing legislation enacted by the U.S. Congress? What option do they have?
Also, why is the Obama Administration so ready to heap praises upon the drug companies, all of which have reaped whirlwind, virtually ensured profits at the expense of the American public that has been denied access to the health benefits provided by access to vital medicines because it must pay the highest cost in the world for its prescription medicines?
But, it is an ill-wind that blows no good. Last Fall, before the elections, a group of advocates for senior advocacy groups from areas across the country, met in Washington, DC to shape support for personal importation of prescription medicines from Tier One countries. At that time, the participants reached a consensus that the importation concept should be included as a part of discussion about comprehensive healthcare reform, a ‘third-leg’ of the stool, because such access to vital medicines is essential to the health and well-being of Americans. It also urged consideration of the beneficial budgetary impact that could be provided though the inclusion of personal importation of prescription medicines into Part D thereby remedying plan shortcomings while saving money for the elderly, protecting their health and creating real savings for the Plan.
Sources tell us that moves have made recently by supporters of importation to define a stronger argument for importation of prescription medicines within the framework of the healthcare debate. We applaud such action. Now, there is an additional opportunity to address the benefits of improved health and savings by fine-tuning the healthcare debate to explore other opportunities for personal importation and defining a role for personal importation in Medicare Part D. Senators Dorgan and Snowe, the two legislators most identified with importation, have issued a statement that reflects their realization that the pharma 'offer' really does not address the challenge of lowering prescription drug prices. And, already, there is a growing realization that the pharmaceutical industry's motives are self-serving.
It is time to call out the pharmaceutical industry. There are legitimate questions that deserve answers about the motives of pharma. It has reaped the benefits of guaranteed pricing for Part D that has led to windfall profits. The claimed or hoped-for savings,while beneficial to individuals, is too little-too late for many elderly. As to the claimed savings to be scored by the Congressional Budget Office, there is a growing realization that possible trade-offs to gain pharma support might actually lead to increased--and virtually guaranteed--sales and earnings.
There is a role for personal importation in helping provide a solution to providing safe, affordable prescription medicines for all Americans. We believe the pharma moves should lead to increased discussion of creating such access, free of what we believe to be unnecessary delays by empowering Secretary Sebelius to designate Tier One countries whose standards of oversight, safety, and efficacy meet of exceed those of the U.S.
Tuesday, June 16, 2009
Dorgan-Snowe needs changes (Chapter 2)
Summary: Earlier, Daniel Hines, publisher of www.TodaysSeniorsNetwork.com and a long-time and continuing supporter of personal importation of safe, affordable prescription medicines from pharmacies in Tier One countries, expresses concerns about current limitations on personal importation in U.S. Senate Bill 525, popularly referred to as Dorgan-Snowe, and urged supporters and sponsors to consider ramifications of the proposed legislation upon access to prescription medicines via the Internet or mail-order—access, which ironically might actually be decreased because of changes in the operations of those pharmacies created by the legislation, sources of supply, and a need to adapt the legislation to the challenges and opportunities that personal importation can provide.In this post, he deals with specific issues:
(1) Importation of medicines is an established fact. The right of individuals to make purchases via importation is established by the fact that a medicine that is unaffordable is unavailable, and Americans therefore have the right to make such purchases. The support on behalf of such access was the result of a classic populist movement by Americans, primarily the elderly, against the predatory pricing practices of pharmaceutical companies.
(2) The bill as presented fails to address the important role of access to prescription medicines as a part of the tremendous opportunity to be a part of comprehensive healthcare reform, and is instead a ‘stand-alone’ bill. This is evidenced by the fact that while drafts of healthcare reform bills such as that of Senator Ted Kennedy (D-MA) have a brief mention of access to prescription medicines as a part of vital healthcare for all Americans, no mention is made of the potential contribution and benefit that could be made by expanded access to safe, affordable prescription medicines from licensed, registered pharmacies in Tier One countries. The supporters of importation on The Hill have missed a tremendous opportunity to establish a presence for importation of medicines to be integrated into the discussion over opportunities for importation of prescription medicines as a part of comprehensive healthcare reform.
(3) One of the biggest challenges facing elderly Americans is the tremendous price increases of prescription medicines in Part D and the larger ‘Doughnut Hole’ in which seniors in the plan are forced to pay out-of-pocket for their prescriptions, while still paying a premium for coverage they are not receiving until their out-of-pocket expenditures reach the catastrophic level. Many never do. That is why we supported the bill introduced in the last Congress by Representative Dennis Kucinich (D-OH) to include imported medicines into the choices for Part D recipients, and why many advocates of importation believe that, properly constructed, there is an opportunity for importation to not only serve the health needs of Americans, but to contribute to budget savings. Yet, there is no provision at this stage of the healthcare reform debate that is just evolving about such a role for importation as an element of Part D, another opportunity lost.
(4) The legislation does not address issues of sourcing of medicines from Canadian pharmacies that reflect changes over the years in Canadian pharmacy operating models. Instead, there is a trapdoor that will stop Dorgan-Snowe from reaching its hoped-for goals because in its first year it limits personal importation of medicines to those from Canadian pharmacies with the medicines coming from Canada only. This in spite of the fact that there are estimates that as much as 80 percent of the prescriptions being fulfilled by Canadian pharmacies comes from Tier One countries whose standards meet or exceed those of the U.S.. But these will not be allowed to be imported into the U.S. by Canadian pharmacies, even though large numbers of Americans are currently doing so, enjoying the health benefits of access to vital medicines that are safe and affordable.
(5) The safety of medicines from pharmacies in Tier One countries such as Australia, New Zealand, the European Community and Japan is an established fact. Ironically, they will be designated for purchase by U.S. consumers after the first year of the limitation in (2), but only from U.S. pharmacies or wholesalers. Why is there a year-wait for such access, particularly in light of the probable shortage of medicines available from Canadian pharmacies because they will be unable to fulfill orders by utilizing sourcing from those same countries?
(6) How eager are Canadian pharmacies to be the engine that drives Dorgan-Snowe? Projections of anticipated revenues by policy-makers fail to account for the possible loss of sales by Canadian pharmacies that will lose access to medicines from Tier One countries as noted above. More significantly, the tremendous drop in the number of mail-order or Internet pharmacies in Canada will have an impact on the funding of importation. The Canadian International Pharmacy Association reportedly has 21 members, a far cry from the 140 pharmacies cited by Senator Charles Grassley (R-IA) that he counts on to generate the sales and the revenues that will contribute to the implementation and administration of Dorgan-Snowe. Over the years, there has been a concern expressed by Canadian pharmacies and Canadian policy-makers over ‘bulk shipments’ to the U.S. Many Canadian authorities fear a scenario in which Canada becomes ‘America’s Drug Store.’ Although when wholesale shipments are authorized in a year there will be the opportunity for shipments to pharmacies and wholesalers in this country from sources other than Canada, what might be the impact if Canadian officials fear a loss of access to medicines for their own citizens? Perception molds reality. Also, how may Canadian pharmacies will choose to participate in Dorgan-Snowe, with its registration fees, posting a $1 million bond, and seeing their margins reduced by other fees based on sales? If they choose not to participate, but continue sales to U.S. citizens, how will the provisions of the bill be enforced? Will they be declared ‘bogus’ pharmacies even though they are operating under the jurisdiction of their particular Provinces? The risk is that untold numbers of Americans might be denied vital medicines, with possible severe health consequences.
(7) How will Americans replace the medicines from other Tier One countries such as Australia, New Zealand, Great Britain, Japan and the European Community that they are now receiving through individual purchases from legitimate, authorized pharmacies that are already complying with standards in their countries that meet or exceed those of the U.S.? These are medicines that are now available but which might be denied for twelve months. Why should there be a year-long wait to establish the arrangements for wholesalers and pharmacies that might want to establish U.S.-based operations to import medicines or to administer plans to provide huge numbers of U.S. citizens the health benefit of access to safe, affordable medicines, access which would otherwise might be denied. Why, when the safety and efficacy of these medicines is already proven, and will be accepted in a year by the U.S., should Americans be denied the ability to make such purchases individually at this or any other time?
(8) The safety of imported medicines from legitimate pharmacies is a fact of life. There are, as far as I have been able to ascertain, no recorded deaths from medicines imported by individuals from legitimate, authorized pharmacies outside the U.S. Sadly, the same cannot be said of medicines from U.S. pharmacies. As a writer for The American Enterprise Institute, hardly a friend of importation, noted: “Only the stupid, lazy or woefully uninformed," would purchase medicine from a bogus pharmacy,” citing the many reliable sources to utilize to verify the safety of pharmacies. As noted, it is a fact that legitimate, authorized pharmacies in a Tier One country of origin must meet standards that meet or exceed those of the U.S. And, all anyone has to do to verify a Canadian pharmacy is to visit the web site of The Canadian International Pharmacy Association. The tragedy of persons buying from counterfeit pharmacies is undeniable. But, no legitimate pharmacy will make a shipment without a physician’s prescription, nor will it ship a controlled substance. Ironically, Google alerts for prescription medicine prices, which once were reliable sources of news about pharmaceutical industry and medicines events and trends, now include numerous mention to ‘pharmacies’ selling a number of drugs—usually Viagra and related medicines—with no prescription required, a sure tip-off to an illicit pharmacy and proof that no amount of regulation can completely stop someone from purchasing from such operations. Common sense and individual responsibility have a role to play. Rather than limiting access to legitimate pharmacies, Dorgan-Snowe should expand it.
(9) The bill lacks the transparency that more citizen involvement could provide. The claim is made on the one hand that the reason for not having hearings on the bill’s proposed language is that it is virtually the same bill that has been offered in the past so there is no need for Congressional hearings. Even granting the validity of this, the fact remains that the circumstances surrounding the bill have changed. Dorgan-Snowe is a bill that, when the importation issue first arose, had defining purposes—safety, efficacy of drugs, improved public health and lower costs for medicines It was a recognition by the supporters of importation that there were benefits to be obtained from allowing Americans access to safe, affordable prescription medicines from other countries, but that there was also a need to reassure patients and families that the proper oversight would be provided to help them identify pharmacies offering those medicines. What have changed are the forces of importation, forces that will shape and determine the success of providing safe, affordable medicines to Americans , not merely measured by passage of the bill.
These forces are described above. But, for importation of medicines to achieve its hoped-for benefits of improved health and well-being of Americans through access to a regimen of vital medicines, some ‘old ground’ will have to be gone over again. We encourage the policy-makers inside the Beltway to welcome the opportunity for additional input and fine-tuning of Dorgan-Snowe that will ensure the success of the legislation for which they have worked so hard for so long. Without such consideration, the consequences might be that the legislation might actually have an impact completely opposite of what is hoped for and cause a reduction in the ability of Americans to benefit from access to safe, affordable imported medicines.
(1) Importation of medicines is an established fact. The right of individuals to make purchases via importation is established by the fact that a medicine that is unaffordable is unavailable, and Americans therefore have the right to make such purchases. The support on behalf of such access was the result of a classic populist movement by Americans, primarily the elderly, against the predatory pricing practices of pharmaceutical companies.
(2) The bill as presented fails to address the important role of access to prescription medicines as a part of the tremendous opportunity to be a part of comprehensive healthcare reform, and is instead a ‘stand-alone’ bill. This is evidenced by the fact that while drafts of healthcare reform bills such as that of Senator Ted Kennedy (D-MA) have a brief mention of access to prescription medicines as a part of vital healthcare for all Americans, no mention is made of the potential contribution and benefit that could be made by expanded access to safe, affordable prescription medicines from licensed, registered pharmacies in Tier One countries. The supporters of importation on The Hill have missed a tremendous opportunity to establish a presence for importation of medicines to be integrated into the discussion over opportunities for importation of prescription medicines as a part of comprehensive healthcare reform.
(3) One of the biggest challenges facing elderly Americans is the tremendous price increases of prescription medicines in Part D and the larger ‘Doughnut Hole’ in which seniors in the plan are forced to pay out-of-pocket for their prescriptions, while still paying a premium for coverage they are not receiving until their out-of-pocket expenditures reach the catastrophic level. Many never do. That is why we supported the bill introduced in the last Congress by Representative Dennis Kucinich (D-OH) to include imported medicines into the choices for Part D recipients, and why many advocates of importation believe that, properly constructed, there is an opportunity for importation to not only serve the health needs of Americans, but to contribute to budget savings. Yet, there is no provision at this stage of the healthcare reform debate that is just evolving about such a role for importation as an element of Part D, another opportunity lost.
(4) The legislation does not address issues of sourcing of medicines from Canadian pharmacies that reflect changes over the years in Canadian pharmacy operating models. Instead, there is a trapdoor that will stop Dorgan-Snowe from reaching its hoped-for goals because in its first year it limits personal importation of medicines to those from Canadian pharmacies with the medicines coming from Canada only. This in spite of the fact that there are estimates that as much as 80 percent of the prescriptions being fulfilled by Canadian pharmacies comes from Tier One countries whose standards meet or exceed those of the U.S.. But these will not be allowed to be imported into the U.S. by Canadian pharmacies, even though large numbers of Americans are currently doing so, enjoying the health benefits of access to vital medicines that are safe and affordable.
(5) The safety of medicines from pharmacies in Tier One countries such as Australia, New Zealand, the European Community and Japan is an established fact. Ironically, they will be designated for purchase by U.S. consumers after the first year of the limitation in (2), but only from U.S. pharmacies or wholesalers. Why is there a year-wait for such access, particularly in light of the probable shortage of medicines available from Canadian pharmacies because they will be unable to fulfill orders by utilizing sourcing from those same countries?
(6) How eager are Canadian pharmacies to be the engine that drives Dorgan-Snowe? Projections of anticipated revenues by policy-makers fail to account for the possible loss of sales by Canadian pharmacies that will lose access to medicines from Tier One countries as noted above. More significantly, the tremendous drop in the number of mail-order or Internet pharmacies in Canada will have an impact on the funding of importation. The Canadian International Pharmacy Association reportedly has 21 members, a far cry from the 140 pharmacies cited by Senator Charles Grassley (R-IA) that he counts on to generate the sales and the revenues that will contribute to the implementation and administration of Dorgan-Snowe. Over the years, there has been a concern expressed by Canadian pharmacies and Canadian policy-makers over ‘bulk shipments’ to the U.S. Many Canadian authorities fear a scenario in which Canada becomes ‘America’s Drug Store.’ Although when wholesale shipments are authorized in a year there will be the opportunity for shipments to pharmacies and wholesalers in this country from sources other than Canada, what might be the impact if Canadian officials fear a loss of access to medicines for their own citizens? Perception molds reality. Also, how may Canadian pharmacies will choose to participate in Dorgan-Snowe, with its registration fees, posting a $1 million bond, and seeing their margins reduced by other fees based on sales? If they choose not to participate, but continue sales to U.S. citizens, how will the provisions of the bill be enforced? Will they be declared ‘bogus’ pharmacies even though they are operating under the jurisdiction of their particular Provinces? The risk is that untold numbers of Americans might be denied vital medicines, with possible severe health consequences.
(7) How will Americans replace the medicines from other Tier One countries such as Australia, New Zealand, Great Britain, Japan and the European Community that they are now receiving through individual purchases from legitimate, authorized pharmacies that are already complying with standards in their countries that meet or exceed those of the U.S.? These are medicines that are now available but which might be denied for twelve months. Why should there be a year-long wait to establish the arrangements for wholesalers and pharmacies that might want to establish U.S.-based operations to import medicines or to administer plans to provide huge numbers of U.S. citizens the health benefit of access to safe, affordable medicines, access which would otherwise might be denied. Why, when the safety and efficacy of these medicines is already proven, and will be accepted in a year by the U.S., should Americans be denied the ability to make such purchases individually at this or any other time?
(8) The safety of imported medicines from legitimate pharmacies is a fact of life. There are, as far as I have been able to ascertain, no recorded deaths from medicines imported by individuals from legitimate, authorized pharmacies outside the U.S. Sadly, the same cannot be said of medicines from U.S. pharmacies. As a writer for The American Enterprise Institute, hardly a friend of importation, noted: “Only the stupid, lazy or woefully uninformed," would purchase medicine from a bogus pharmacy,” citing the many reliable sources to utilize to verify the safety of pharmacies. As noted, it is a fact that legitimate, authorized pharmacies in a Tier One country of origin must meet standards that meet or exceed those of the U.S. And, all anyone has to do to verify a Canadian pharmacy is to visit the web site of The Canadian International Pharmacy Association. The tragedy of persons buying from counterfeit pharmacies is undeniable. But, no legitimate pharmacy will make a shipment without a physician’s prescription, nor will it ship a controlled substance. Ironically, Google alerts for prescription medicine prices, which once were reliable sources of news about pharmaceutical industry and medicines events and trends, now include numerous mention to ‘pharmacies’ selling a number of drugs—usually Viagra and related medicines—with no prescription required, a sure tip-off to an illicit pharmacy and proof that no amount of regulation can completely stop someone from purchasing from such operations. Common sense and individual responsibility have a role to play. Rather than limiting access to legitimate pharmacies, Dorgan-Snowe should expand it.
(9) The bill lacks the transparency that more citizen involvement could provide. The claim is made on the one hand that the reason for not having hearings on the bill’s proposed language is that it is virtually the same bill that has been offered in the past so there is no need for Congressional hearings. Even granting the validity of this, the fact remains that the circumstances surrounding the bill have changed. Dorgan-Snowe is a bill that, when the importation issue first arose, had defining purposes—safety, efficacy of drugs, improved public health and lower costs for medicines It was a recognition by the supporters of importation that there were benefits to be obtained from allowing Americans access to safe, affordable prescription medicines from other countries, but that there was also a need to reassure patients and families that the proper oversight would be provided to help them identify pharmacies offering those medicines. What have changed are the forces of importation, forces that will shape and determine the success of providing safe, affordable medicines to Americans , not merely measured by passage of the bill.
These forces are described above. But, for importation of medicines to achieve its hoped-for benefits of improved health and well-being of Americans through access to a regimen of vital medicines, some ‘old ground’ will have to be gone over again. We encourage the policy-makers inside the Beltway to welcome the opportunity for additional input and fine-tuning of Dorgan-Snowe that will ensure the success of the legislation for which they have worked so hard for so long. Without such consideration, the consequences might be that the legislation might actually have an impact completely opposite of what is hoped for and cause a reduction in the ability of Americans to benefit from access to safe, affordable imported medicines.
Subscribe to:
Posts (Atom)